

The role of indocyanine green in fluorescence-guided pancreatic surgery: a comprehensive review
- PMID: 40009558
- PMCID: PMC12165567
- DOI: 10.1097/JS9.0000000000002311
The role of indocyanine green in fluorescence-guided pancreatic surgery: a comprehensive review
Abstract
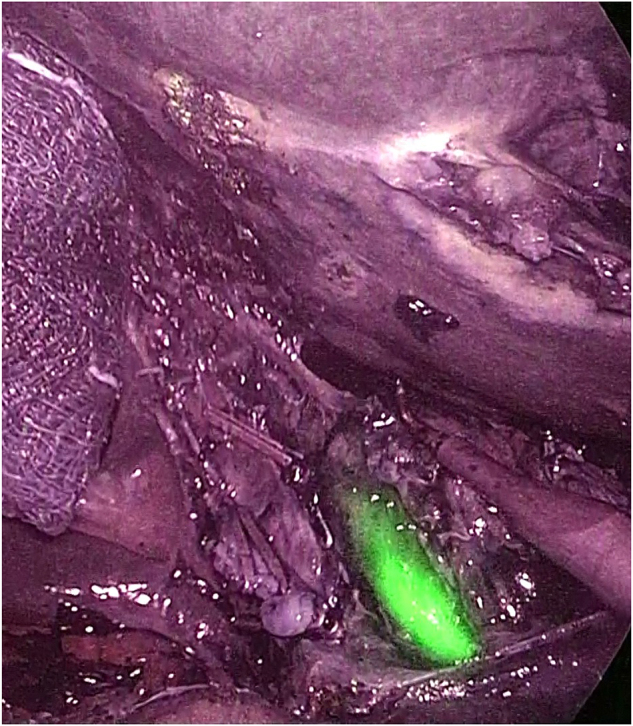
Pancreatic surgery is a complex and challenging field, with patients facing a high risk of postoperative complications. In recent years, indocyanine green (ICG) has gained prominence as a valuable tool used in various aspects of pancreatic surgery. ICG is a fluorescent dye that offers real-time imaging capabilities that enhance the surgeon's ability to accurately localize tumors and critical anatomical structures, thereby improving surgical precision and potentially reducing operative time and complications. One of the most significant advantages of ICG is its ability to provide enhanced visualization of the biliary tract and vascular structures, which is particularly beneficial in complex pancreatic resections, in which the anatomy can be highly variable and challenging to navigate. Furthermore, ICG can be instrumental in ensuring the adequate perfusion of anastomoses, thereby reducing the risk of postoperative leaks and associated morbidity. This comprehensive review aims to provide an in-depth analysis of the current applications, advantages, and limitations of ICG in pancreatic surgery.
Keywords: indocyanine green; mininvasive surgery; pancreas surgery; pancreatic cancer; precision surgery.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc.
Figures

References
-
- Ohtsuka T, Nagakawa Y, Toyama H, et al. A multicenter prospective registration study on laparoscopic pancreatectomy in Japan: report on the assessment of 1,429 patients. J Hepatobiliary Pancreat Sci 2020;27:47–55. - PubMed
-
- International Study Group on Minimally Invasive Pancreas Surgery (I-MIPS). Asbun HJ, Moekotte AL, Vissers FL, et al. The Miami International Evidence-based Guidelines on minimally invasive pancreas resection. Ann Surg 2020;271:1–14. - PubMed
-
- Wang X, Teh CSC, Ishizawa T, et al. Consensus guidelines for the use of fluorescence imaging in hepatobiliary surgery. Ann Surg 2021;274:97–106. - PubMed
-
- Ij FOX, Brooker LG, Heseltine DW, Essex HE, Wood EH. A tricarbocyanine dye for continuous recording of dilution curves in whole blood independent of variations in blood oxygen saturation. Proc Staff Meet Mayo Clin 1957;32:478–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
