

Evolution of SARS-CoV-2 antibody repertoire after successive mRNA vaccinations under immunosuppressive treatment
- PMID: 40010153
- PMCID: PMC11905820
- DOI: 10.1016/j.ebiom.2025.105620
Evolution of SARS-CoV-2 antibody repertoire after successive mRNA vaccinations under immunosuppressive treatment
Abstract
Background: Repeated antigen exposure can result in a shifting antibody repertoire. The mechanisms by which this occurs and consequences for cross-variant protection against evolving pathogens remain incompletely understood, particularly in the context of immunosuppressive treatments used in patients with immune-mediated inflammatory diseases (IMID).
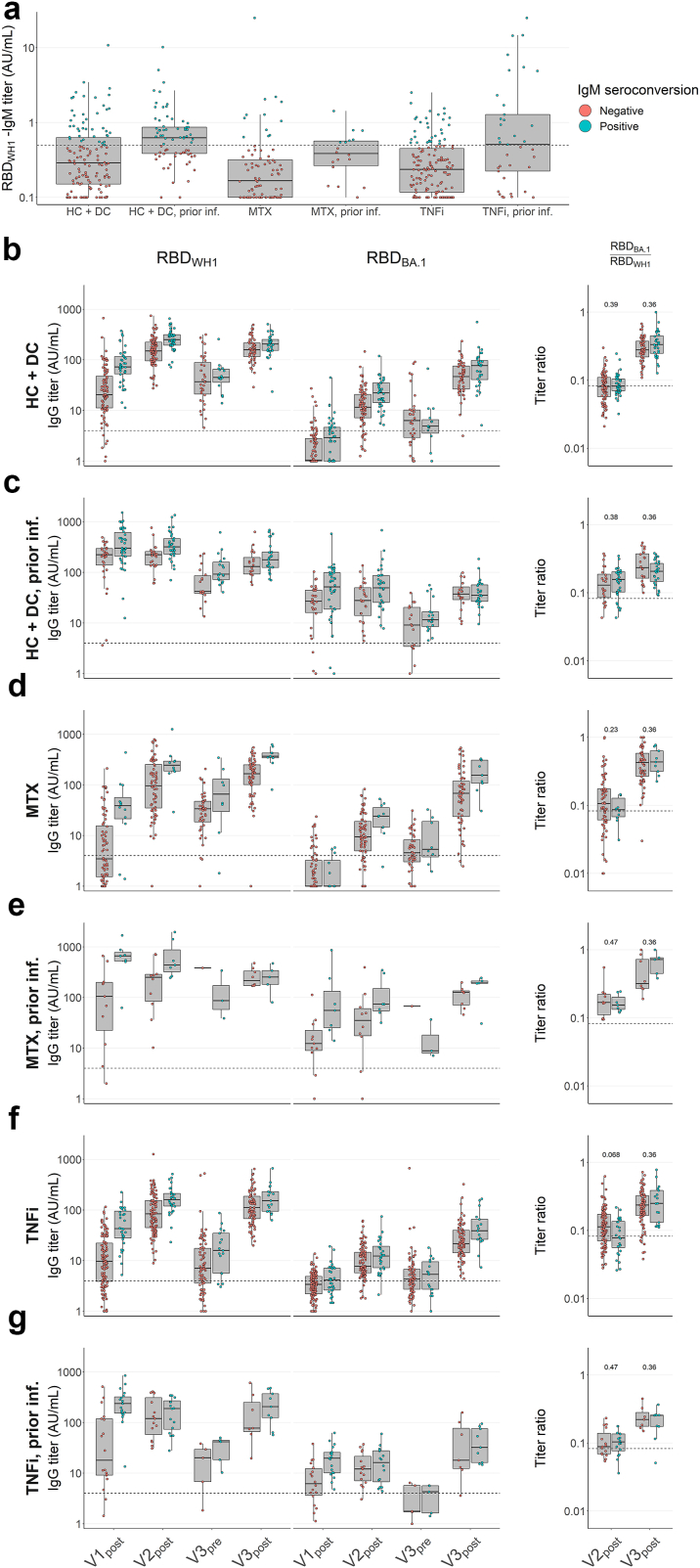
Methods: To investigate this, we characterised longitudinal changes in the anti-SARS-CoV-2 antibody repertoire over the course of three SARS-CoV-2 mRNA vaccinations in patients with IMIDs treated with methotrexate (MTX) and/or tumour necrosis factor-inhibitors (TNFi), anti-CD20 monoclonal antibodies, no systemic therapy, and healthy controls (total N = 878). We determined serum antibody titres against the receptor-binding domain (RBD) of Wuhan-Hu-1 (WH1) and Omicron BA.1 spike proteins, and assessed ratios thereof between groups as a proxy for cross-reactivity.
Findings: We observe emerging anti-BA.1 RBD reactivity over time, notably following a third vaccination. This may be partly explained by affinity maturation, as evaluated by inhibition of ACE2-RBD interactions. Similar trends were seen in patients treated with MTX and/or TNFi, but not in patients on anti-CD20 therapy. SARS-CoV-2 infection prior to vaccination accelerated these effects initially while leading to comparable results after three vaccinations.
Interpretation: MTX and TNFi do not qualitatively alter the evolution of the antibody repertoire in response to repeated antigen exposure, whereas anti-CD20 does. These insights may help to optimise vaccination strategies for patients with immune-mediated inflammatory diseases.
Funding: This study was supported by ZonMw (The Netherlands Organization for Health Research and Development) and SGF (Collaborating Health Funds).
Keywords: Antibody repertoire; Autoimmune disease; SARS-CoV-2; Serology; mRNA vaccines.
Copyright © 2025 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests For funding of this study, SMvH, FE, TWK and TR report grants from ZonMw and SMvH reports a grant from SGF to study immune responses after SARS-Cov-2 vaccination in autoimmune diseases. JK reports grants for multicentre investigator-initiated trials from ZonMw and Treatmeds; contracted research grants to his institution from F. Hoffmann-La Roche Ltd, Biogen, Immunic, Teva, Merck, Novartis and Sanofi/Genzyme; speaker's fees paid to his institution from F. Hoffmann-La Roche Ltd, Biogen, Immunic, Teva, Merck, Novartis and Sanofi/Genzyme; and compensation paid to his institution for participation in an adjudication committee of an MS clinical trial by Immunic. SWT reports grants paid to his institution from GlaxoSmithKline, Pfizer, Roche, AstraZeneca and Galapagos; and speaker's fees paid to his institution from NovoNordisk, AbbVie and UCB. SMvH reports compensation paid to her institution for participation in EU member expert panel HORIZON-HLTH-2023-DISEASE-03-18 and in the supervisory board of EU consortium INsTRuCT, from EU Horizon 2020 grants; unpaid participation in the supervisory board of national consortium DC4BALANCE, in the board of the European Federation of Immunological Societies, as co-project leader of ZonMw COVID-19 research program “Immunity against SARS-CoV-2 in immune-suppressed patients: increased risk of insufficient immunological memory or sufficient protection against re-infection?”, and in the project management board of national consortium ImmuneHealthSeed. FE reports grants from Prinses Beatrix Spierfonds, CSL Behring, Kedrion, Terumo BCT, Grifols, Takeda Pharmaceutical Company, and GBS-CIDP Foundation; consulting fees from UCB Pharma and CSL Behring; and honoraria from Grifols. All other authors declare no competing interests.
Figures





References
-
- Baden L.R., El Sahly H.M., Essink B., et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med. 2021;384(5):403–416. http://www.nejm.org/doi/10.1056/NEJMoa2035389 Available from: - DOI - PMC - PubMed
-
- Polack F.P., Thomas S.J., Kitchin N., et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383(27):2603–2615. http://www.nejm.org/doi/10.1056/NEJMoa2034577 Available from: - DOI - PMC - PubMed
-
- Wang L., Cheng G. Sequence analysis of the emerging SARS-CoV-2 variant Omicron in South Africa. J Med Virol. 2022;94(4):1728–1733. https://onlinelibrary.wiley.com/doi/10.1002/jmv.27516 Available from: - DOI - PubMed
-
- Majumdar S., Sarkar R. Mutational and phylogenetic analyses of the two lineages of the Omicron variant. J Med Virol. 2022;94(5):1777–1779. https://onlinelibrary.wiley.com/doi/10.1002/jmv.27558 Available from: - DOI - PMC - PubMed
-
- Muecksch F., Wang Z., Cho A., et al. Increased memory B cell potency and breadth after a SARS-CoV-2 mRNA boost. Nature. 2022;607(7917):128–134. http://www.ncbi.nlm.nih.gov/pubmed/35447027 Available from: - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
