

Efficacy of endoscopic ultrasound-guided biliary drainage of malignant biliary obstruction: a systematic review and meta-analysis of randomized controlled trials
- PMID: 40010703
- PMCID: PMC12314615
- DOI: 10.5946/ce.2024.183
Efficacy of endoscopic ultrasound-guided biliary drainage of malignant biliary obstruction: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Malignant biliary obstruction is a major clinical challenge. We assessed the efficacy of endoscopic ultrasound-guided biliary drainage (EUS-BD) compared with that of endoscopic retrograde cholangiopancreatography biliary drainage (ERCP-BD) or percutaneous transhepatic biliary drainage (PTBD).
Methods: We searched for randomized controlled trials comparing EUS-BD with ERCP or PTBD in treating malignant biliary obstruction. Using random-effects models, we synthesized risk ratios (RRs) and weighted mean differences (WMDs) with 95% confidence intervals (CIs). A subgroup analysis was performed using a comparator (ERCP or PTBD).
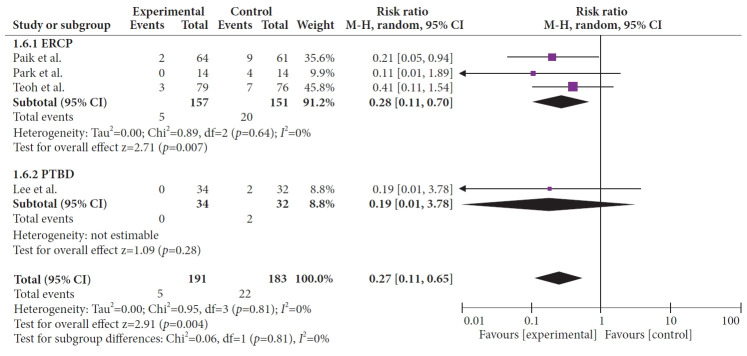
Results: EUS-BD significantly reduced the risk of stent dysfunction (RR, 0.46; 95% CI, 0.33-0.64), with consistent results in subgroup analysis for ERCP (RR, 0.54; 95% CI, 0.35-0.84) and PTBD (RR, 0.37; 95% CI, 0.22-0.61). It also lowered the risk of post-procedure pancreatitis (RR, 0.24; 95% CI, 0.07-0.83) and reduced tumor ingrowth or overgrowth risk (RR, 0.27; 95% CI, 0.11-0.65), even when compared to ERCP alone (RR, 0.28; 95% CI, 0.11-0.70). EUS-BD demonstrated a lower risk of adverse events compared to PTBD (RR, 0.37; 95% CI, 0.14-0.97) and reduced length of hospital stay (WMD, -1.03; 95% CI, -1.53 to -0.53) when compared to ERCP.
Conclusions: EUS-BD outperformed ERCP-BD and PTBD in reducing stent dysfunction, postprocedural pancreatitis, and tumor ingrowth or overgrowth.
Keywords: Biliary tract diseases; Endoscopic retrograde cholangiopancreatography; Endoscopy; Meta-analysis.
Conflict of interest statement
The authors have no potential conflicts of interest.
Figures





References
-
- Artifon EL, Aparicio D, Paione JB, et al. Biliary drainage in patients with unresectable, malignant obstruction where ERCP fails: endoscopic ultrasonography-guided choledochoduodenostomy versus percutaneous drainage. J Clin Gastroenterol. 2012;46:768–774. doi: 10.1097/mcg.0b013e31825f264c. - DOI - PubMed
LinkOut - more resources
Full Text Sources
