

Network meta-analysis comparing efficacy of different strategies on medication-overuse headache
- PMID: 40011869
- PMCID: PMC11863719
- DOI: 10.1186/s10194-025-01982-9
Network meta-analysis comparing efficacy of different strategies on medication-overuse headache
Erratum in
-
Correction: Network meta‑analysis comparing efficacy of different strategies on medication‑overuse headache.J Headache Pain. 2025 Apr 16;26(1):81. doi: 10.1186/s10194-025-02031-1. J Headache Pain. 2025. PMID: 40240915 Free PMC article. No abstract available.
Abstract
Background: Medication-overuse headache (MOH) is the most common secondary headache disorder, resulting from or leading to the frequent use of acute headache medications. Despite the availability of various treatment strategies, the optimal approach remains uncertain.
Objective: This network meta-analysis (NMA) aimed to evaluate the comparative efficacy of different strategies for managing MOH, focusing on reducing monthly headache days.
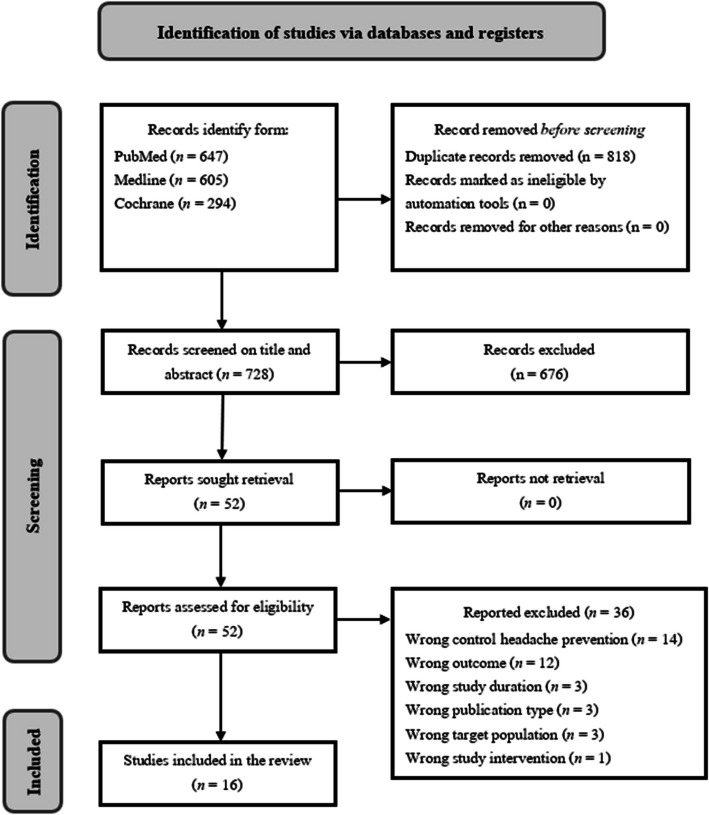
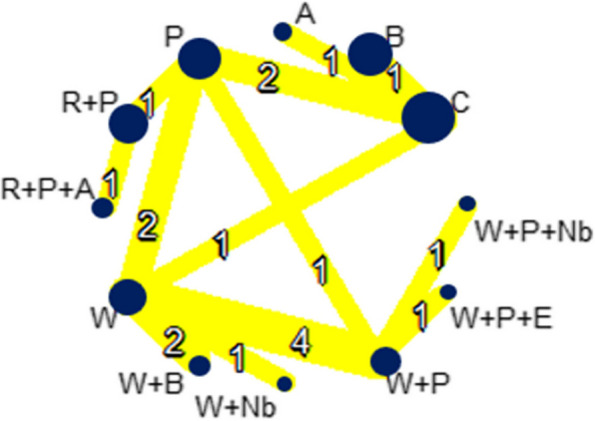
Methods: We systematically reviewed randomized controlled trials (RCTs) comparing withdrawal strategies, including bridging therapies, the use of concurrent migraine prevention drugs, and additional education, in adult patients diagnosed with MOH. The primary outcome was the reduction in monthly headache days. Eligible studies were analyzed using a random-effects NMA model, integrating both direct and indirect evidence. Treatments were ranked using p-scores, and risk of bias was assessed using the Cochrane risk of bias tool 2.0.
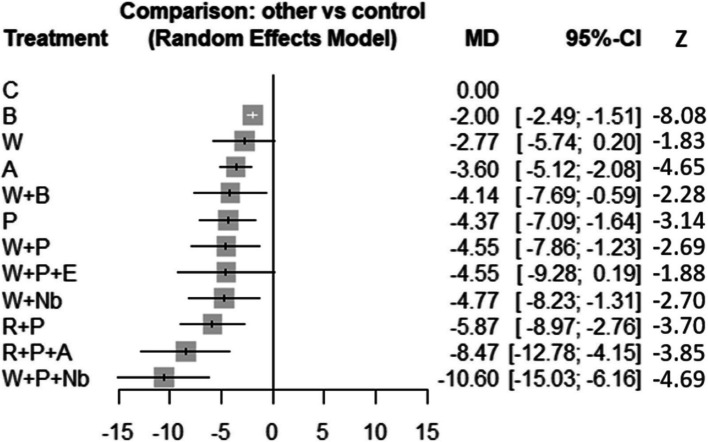
Results: Sixteen RCTs involving 3,000 participants were included. Compared to control, combination therapies, such as abrupt withdrawal with oral prevention and greater occipital nerve block and restriction of overused acute medication with oral prevention and Calcitonin gene-related peptide (CGRP) therapies, demonstrated the greatest efficacy, with reductions in monthly headache days of -10.6 (95% CI: [-15.03; -6.16]) and -8.47 (95% CI: [-12.78; -4.15]), respectively. Headache prevention strategies, including oral prevention (P), anti-calcitonin gene-related peptide (receptor) (CGRP(R)) therapies (A), and botulinum toxin (B) showed significant in reduction of monthly headache days, but no single initial prevention strategy demonstrates superior efficacy over the others. In contrast, abrupt withdrawal alone (W) showed no significant efficacy, with a mean difference of -2.77 (95% CI: [-5.74; 0.20]).
Conclusion: Combination therapies, including anti-CGRP(R) therapies and nerve blocks, appear to be the most effective strategies for MOH management, highlighting their potential as initial treatment options. While headache prevention strategies demonstrated similar efficacy, abrupt withdrawal alone was insufficient. The observed reduction in headache frequency after treatment suggests that strategies with greater efficacy may help lower the likelihood of MOH relapse.
Trial registration: PROSPERO, CRD 42024620487.
Keywords: Calcitonin gene-related peptide therapy; Chronic migraine; Medication overuse; Medication-overuse headache.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Headache Classification Committee of the International Headache Society (IHS) (2018) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 38(1):1–211 - PubMed
-
- Westergaard ML, Hansen EH, Glümer C, Olesen J, Jensen RH (2014) Definitions of medication-overuse headache in population-based studies and their implications on prevalence estimates: A systematic review. Cephalalgia 34(6):409–425 - PubMed
-
- De Goffau MJ, Klaver ARE, Willemsen MG, Bindels PJE, Verhagen AP (2017) The Effectiveness of Treatments for Patients With Medication Overuse Headache: A Systematic Review and Meta-Analysis. J Pain 18(6):615–627 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
