

American Society for Gastrointestinal Endoscopy guideline on the diagnosis and management of GERD: methodology and review of evidence
- PMID: 40012897
- PMCID: PMC11852708
- DOI: 10.1016/j.vgie.2024.10.001
American Society for Gastrointestinal Endoscopy guideline on the diagnosis and management of GERD: methodology and review of evidence
Abstract
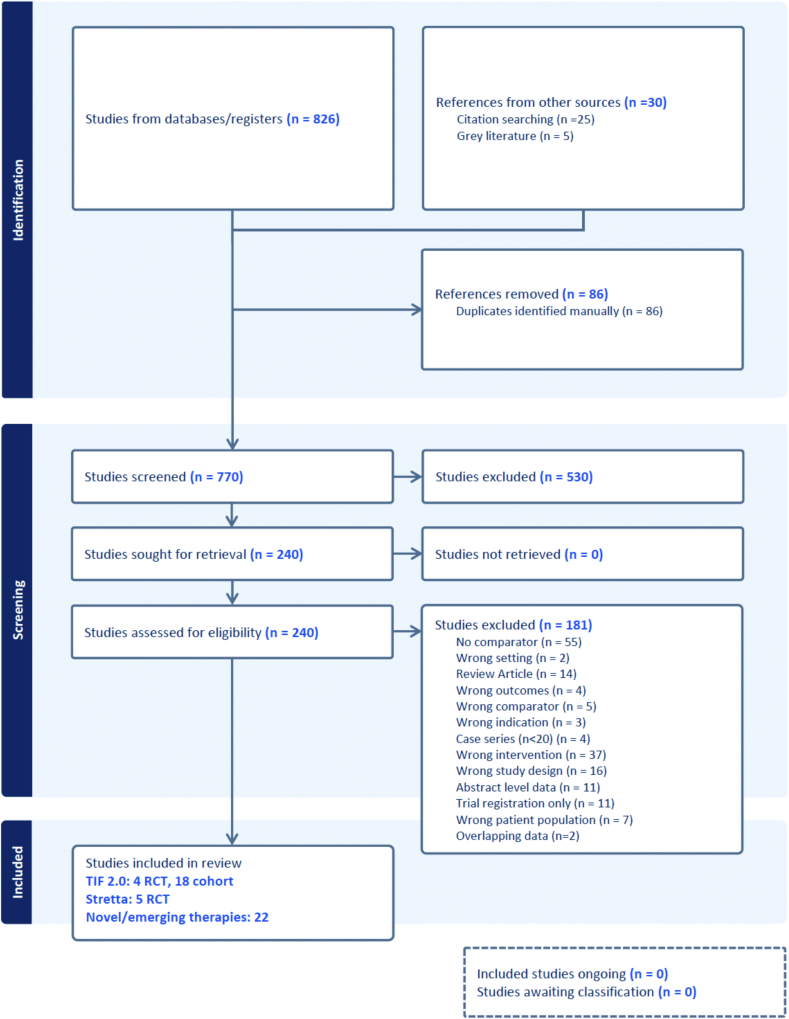
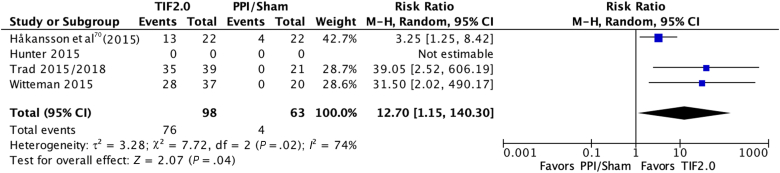
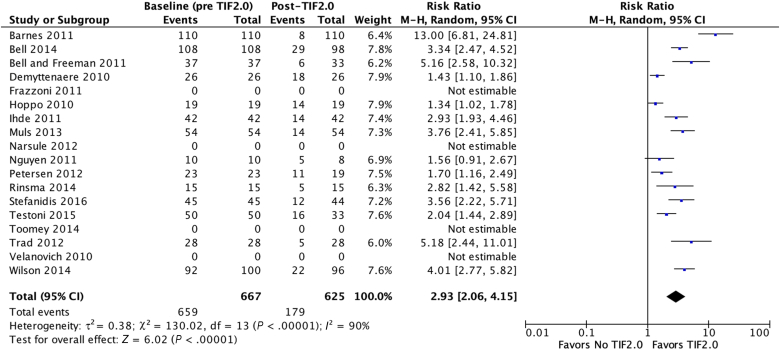
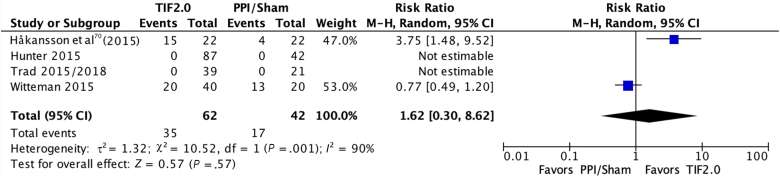
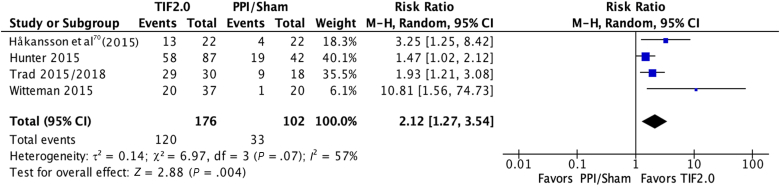
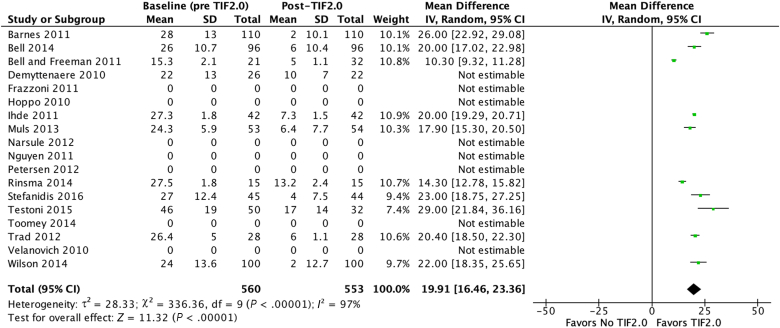
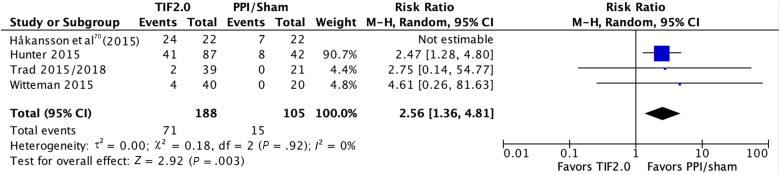
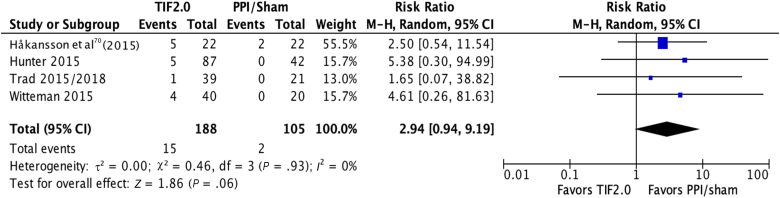
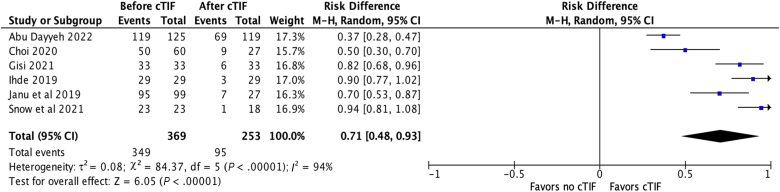
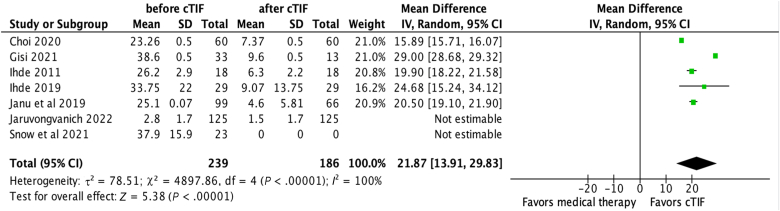
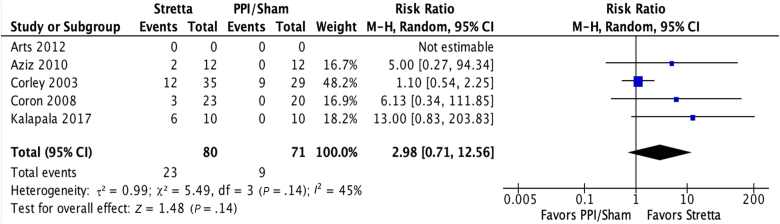
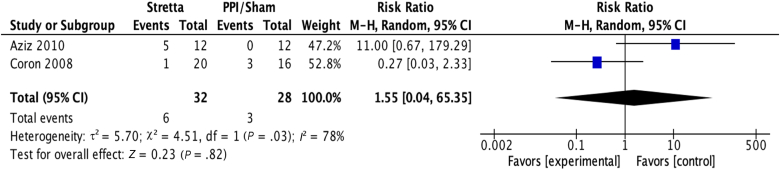
This clinical practice guideline from the American Society for Gastrointestinal Endoscopy (ASGE) provides an evidence-based approach for strategies to diagnose and manage GERD. This document was developed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework and serves as an update to the prior ASGE guideline on the role of endoscopy in the management of GERD (2014). The updated guideline addresses the indications for endoscopy in patients with GERD, including patients who have undergone sleeve gastrectomy (SG) and peroral endoscopic myotomy (POEM). It also discusses endoscopic evaluation of gastroesophageal junctional integrity comprehensively and uniformly. Important, this guideline discusses management strategies for GERD including lifestyle interventions, proton pump inhibitors (PPIs), and endoscopic antireflux therapy including transoral incisionless fundoplication (TIF), radiofrequency energy, and TIF combined with hiatal hernia repair (cTIF). The ASGE recommends upper endoscopy for the evaluation of GERD in patients with alarm symptoms. The ASGE suggests upper endoscopy for symptomatic patients with a history of SG and POEM. The ASGE recommends careful endoscopic evaluation, reporting, and photo-documentation of objective GERD findings and gastroesophageal junction landmarks and integrity to improve patient care and outcomes. In patients with GERD symptoms, the ASGE recommends lifestyle modifications. In patients with symptomatic and confirmed GERD with predominant heartburn symptoms, the ASGE recommends medical management including PPIs at the lowest dose for the shortest duration while initiating discussion about long-term management options. In patients with confirmed GERD with small hiatal hernia (≤2 cm) and Hill grade I or II flap valve who meet specific criteria, the ASGE suggests evaluation for TIF as an alternative to long-term medical management. In patients with confirmed GERD with a large hiatal hernia (>2 cm) and Hill grade 3 or 4 flap valve, the ASGE suggests evaluation for combined endoscopic-surgical TIF (cTIF) in a multidisciplinary review. This document clearly outlines the methodology, analysis, and decision used to reach the final recommendations and represents the official ASGE recommendations on the above topics.
© 2025 by the American Society for Gastrointestinal Endoscopy. Published by Elsevier, Inc.
Conflict of interest statement
N. C. Thosani is a consultant for and has received travel compensation and food and beverage from PENTAX of America, Inc, and Boston Scientific Corporation; is a speaker for and has received travel compensation and food and beverage from AbbVie Inc, and is a consultant for Ambu Inc. A. Saeed is a consultant for Endogastric Solutions, Medtronic, Boston Scientific Corporation, and Olympus. B. Abu Dayyeh is a consultant for Endogenex, Endo-TAGSS, Metamodix, and BFKW; is a consultant for and receives grant or research support from USGI, Apollo Endosurgery, Spatz Medical, Aspire Bariatrics, and Boston Scientific; has speaker roles with Olympus, Johnson and Johnson; is a speaker for and receives grant or research support from Medtronic and Endogastric Solutions; and receives grant support from ERBE Medical. M.I. Canto is a principal investigator on a research grant study with The Johns Hopkins University sponsored by Endogastric Solutions; is a consultant and on the scientific advisory board for Cernostics; has a research grant and clinical trial through Pentax Medical Corporation; was a consultant for ClearNote Health and Cernostics; and receives royalties from UpToDate. W. Abidi is a consultant for and has received food and beverage from Ambu Inc, Apollo Endosurgery US Inc, CONMED Corporation; has received research support from GI Dynamics; and has received food and beverage from Olympus America Inc, AbbVie Inc, Boston Scientific Corporation, RedHill Biopharma Inc, and Salix Pharmaceuticals. S.K. Amateau is a consultant for and has received travel compensation and food and beverage from Boston Scientific Corporation; is a consultant and on the advisory board for Merit Medical; is a consultant and has received food and beverage from Olympus Corporation of the Americas; is a consultant for MTEndoscopy, US Endoscopy, and Heraeus Medical Components, LLC; and is a consultant and has received food and beverage from Cook Medical LLC. N. Cosgrove is a consultant for Olympus Corporation of the Americas; is a consultant and has received food and beverage from Boston Scientific Corporation; and has received food and beverage from Ambu Inc S.E. Elhanafi has received food and beverage from Medtronic, Inc, Nestle HealthCare Nutrition Inc, Ambu Inc, Salix Pharmaceuticals, Takeda Pharmaceuticals U.S.A., Inc, and Merit Medical Systems Inc. N. Forbes has been a consultant for Boston Scientific Corporation and PENTAX of America, Inc; has been on the speaker bureau for PENTAX of America, Inc, and Boston Scientific Corporation; and has received research support from PENTAX of America, Inc D.R. Kohli has been a consultant for and has received a research grant from Olympus Corporation of the Americas. L.L. Fujii-Lau is a consultant for Boston Scientific Corporation and has received food and beverage from Pfizer Inc and AbbVie Inc. J.D. Machicado is a consultant for and has received food and beverage from Mauna Kea Technologies, Inc; and has received food and beverage from Boston Scientific Corporation. N.B. Marya is a consultant for and has received food and beverage from Boston Scientific Corporation; and has received food and beverage from Apollo Endosurgery US Inc S. Ngamruengphong is a consultant for Boston Scientific Corporation, Olympus, and Neptune Medical; and has received food and beverage from Medtronic, Inc, Boston Scientific Corporation, PENTAX of America, Inc, and Ambu Inc S. Pawa is a consultant for Boston Scientific Corporation. N.R. Thiruvengadam has received a grant from Boston Scientific Corporation. B.J. Qumseya is a consultant for and has received food and beverage from Medtronic, Inc; is a consultant for Assertio Management, LLC; is a speaker for Castle Biosciences; and has received food and beverage from FUJIFILM Healthcare Americas Corporation and Boston Scientific Corporation. The other authors disclosed no financial relationships.
Figures









References
-
- Locke G.R., Talley N.J., Fett S.L., Zinsmeister A.R., Melton L.J. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112:1448–1456. - PubMed
-
- Vakil N., van Zanten S.V., Kahrilas P., Dent J., Jones R., Global Consensus Group The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–1920. quiz 1943. - PubMed
-
- Rosen R., Vandenplas Y., Singendonk M., et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2018;66:516–554. - PMC - PubMed
LinkOut - more resources
Full Text Sources
