

Cost-effectiveness of screening for developmental dysplasia of the hip in Karachi, Pakistan using a universally applicable cost-effectiveness model
- PMID: 40018184
- PMCID: PMC11812765
- DOI: 10.1136/bmjph-2023-000340
Cost-effectiveness of screening for developmental dysplasia of the hip in Karachi, Pakistan using a universally applicable cost-effectiveness model
Abstract
Introduction: Developmental dysplasia of the hip (DDH) is a congenital anomaly of the hip socket that can lead to lifelong disability and pain when left untreated. DDH is a good candidate for screening because of its high frequency in population, availability of treatment and the possibility of secondary prevention. Pakistan currently does not have any systematic or universal neonatal screening programme for DDH.
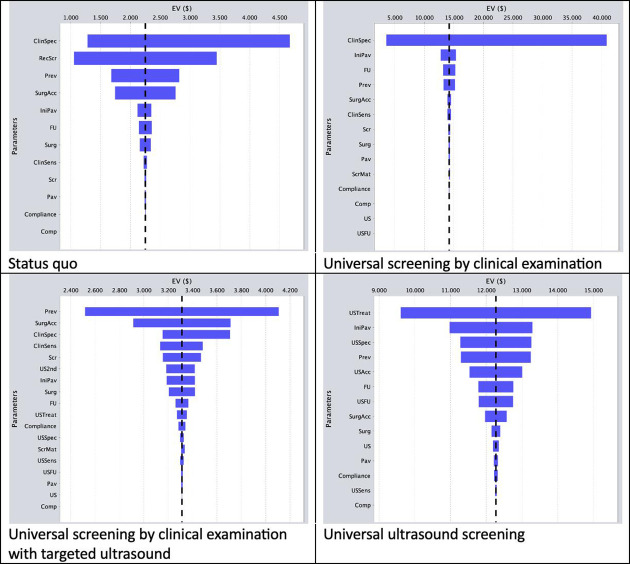
Methods: The cost-effectiveness model in this study uses one decision tree for each screening scenario: (1) the status quo, (2) universal screening by clinical examination, (3) universal screening by clinical examination with targeted ultrasound (US) screening, (4) and universal screening by US. Loss of disability-adjusted life-years (DALYs) is used as outcome variable.
Results: When left untreated DDH creates a loss of 3.4 DALYs per person. Clinical examination and targeted US averts most DALYs per dollar spent. Generalised US averts more DALYs overall but requires a greater financial investment per DALY averted.
Conclusions: Universal US screening reaches more children and can be considered the more equitable approach but requires 10 times the financial investment clinical examination and targeted US requires. The decision which option is most appropriate for Karachi, Pakistan depends on resource availability, geography, infrastructure, treatment capacity, health system values and societal factors in Pakistan.
Keywords: Community Health; Secondary Prevention; economics.
Copyright © Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. Published by BMJ.
Conflict of interest statement
None declared.
Figures


References
-
- Miller M, Thompson S, Hart J. Review of orthopaedics. Sixth Edit. Philadelphia: Elsevier Saunders; 2012. pp. 257–61.
-
- Am A, Saw A, Nawar M. Treatment of developmental dysplasia of the hip: short and mid-term outcome. Malaysian Orthop J . 2011;5:17–20. doi: 10.5704/MOJ.1103.004. - DOI
-
- Shipman S, Helfand M, Nygren P, et al. Screening for developmental dysplasia of the hip. Rockville: Agency for Healthcare Research and Quality (US); 2006. https://www.ncbi.nlm.nih.gov/books/NBK33430/ Available. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials