

Reperfused Myocardial Infarction: The Road to CCS Classification of Acute MI and Beyond
- PMID: 40021272
- PMCID: PMC11905164
- DOI: 10.1016/j.jacadv.2024.101528
Reperfused Myocardial Infarction: The Road to CCS Classification of Acute MI and Beyond
Abstract
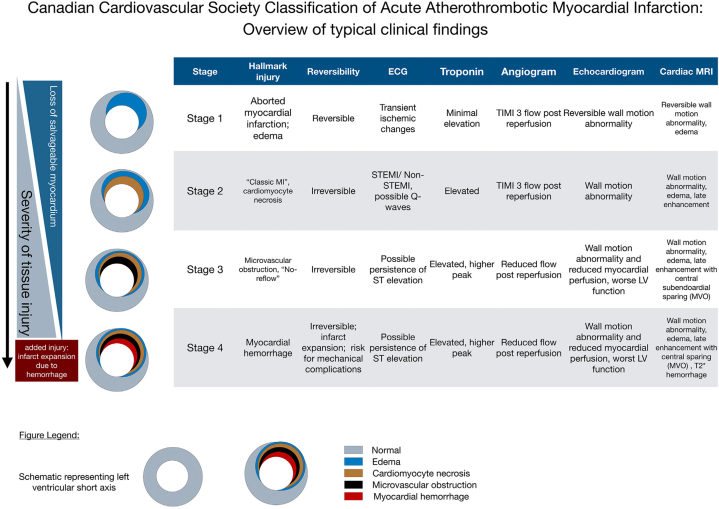
The Canadian Cardiovascular Society recently put forth a new classification of acute reperfused myocardial infarction (MI) based on stages of myocardial injury. Backed by more than 5 decades of intense investigation in the field, the key message of this new classification is that not all MIs are the same and that the type and extent of myocardial injury should be considered in diagnosing and treating MI. We review the literature with the goal of highlighting the progressive advances that enabled the synthesis of the Canadian Cardiovascular Society classification into 4 distinct stages of tissue injury. We emphasize the major breakthroughs from insights gained from experimental, translational, and clinical studies to date. We also identify current gaps in knowledge and critical research directions that need to be pursued to improve patient care and reduce post-MI complications such as chronic heart failure and malignant arrhythmias, whose risk is linked to stage and extent of myocardial injury.
Keywords: CCS stages of myocardial tissue injury; intramyocardial hemorrhage; myocardial infarction; reperfusion injury; reperfusion therapy.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding support and author disclosures This work was funded in part by National Institutes of Health (HL133407, HL136578, and HL147133) to Dr Dharmakumar. Dr Dharmakumar has an ownership interest in Cardio-theranostics, LLC. Dr Kalra is the founding director of makeadent.org Aavishqaar Fund. Dr Kovacs is on the Clinical Events Adjudication Committee for Cook Inc; is on the ECG Adjudication for Eli Lilly; is on the data safety monitoring board for Immunovant and GSK; is a consultant for Jazz and GenInCode; and receives research grant from Pfizer. Dr Henry is a consultant for Corflow. Dr Kumar is an advisor to Cardio-Theranostics, LLC. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures






References
-
- Martin S.S., Aday A.W., Almarzooq Z.I., et al. 2024 heart disease and stroke statistics: a report of US and global data from the American heart association. Circulation. 2024;149:e347–e913. - PubMed
-
- Murugiah K., Wang Y., Nuti S.V., et al. Are non-ST-segment elevation myocardial infarctions missing in China? Eur Heart J Qual Care Clin Outcomes. 2017;3:319–327. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
