

Diagnostic Accuracy Prior to Congenital Heart Defect Surgery: A Multicenter Collaboration
- PMID: 40021273
- PMCID: PMC11905157
- DOI: 10.1016/j.jacadv.2024.101558
Diagnostic Accuracy Prior to Congenital Heart Defect Surgery: A Multicenter Collaboration
Abstract
Background: Echocardiography is the mainstay for diagnosing congenital heart disease (CHD). Diagnostic errors can lead to suboptimal surgical outcomes.
Objectives: This multicenter pediatric echocardiography collaborative learning initiative explores reasons for diagnostic errors, investigates associations between patient- and center-specific factors and errors, and relays the benefits of a multicenter approach to decrease these errors as a first step to improve CHD surgical outcomes.
Methods: Participating centers submitted diagnostic evaluations on patients prior to 2-ventricle repair into a central database. We held virtual meetings to revise variables and discuss cases to learn from each other.
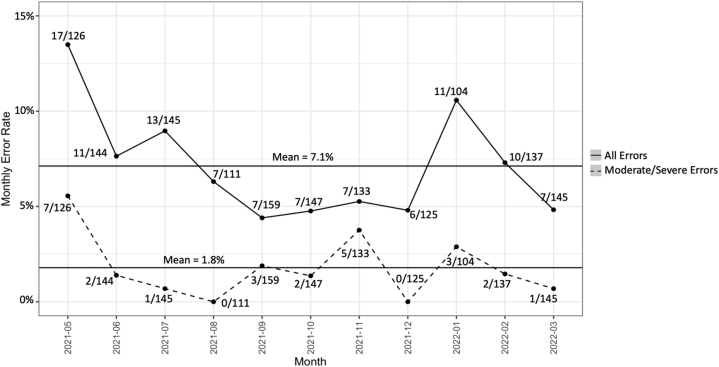
Results: Fourteen pediatric echocardiography laboratories entered data on 1,476 consecutive patients with specific cardiac diagnoses who underwent a two-ventricle repair over 11 months. The mean error rate across centers was 7.1% (103 errors, 17/126-6/125). Seventy-six (74%) errors were preventable or possibly preventable. Cognitive (43%) and imaging factors (47%) commonly contributed to these errors. Moderate to severe impact on postoperative outcomes occurred in 19 (25%) preventable or possibly preventable errors. There were no statistically significant associations between patient- or center-specific factors and errors.
Conclusions: This work represents the feasibility and advantages of a multicenter approach to preoperative diagnostic errors. Variability existed in sedated protocols, number of echos needed, use of other modalities, and in other processes. Common anatomic areas were found. Rather than undertaking isolated, single-center projects, this collaborative is poised to learn about novel changes that would improve diagnostic accuracy across centers as a first step to advancing surgical outcomes for patients with CHD.
Keywords: echocardiography (echo) laboratory (lab); pediatric diagnostic errors; quality improvement (QI).
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding support and author disclosures This work was supported by the Cardiac Center at the Children's Hospital of Philadelphia. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
-
- Gutgesell H.P., Huhta J.C., Latson L.A., Huffines D., McNamara D.G. Accuracy of two-dimensional echocardiography in the diagnosis of congenital heart disease. Am J Cardiol. 1985;55:514–518. - PubMed
-
- Stark J., Smallhorn J., Huhta J., et al. Surgery for congenital heart defects diagnosed with cross-sectional echocardiography. Circulation. 1983;68(suppI II):II123–II138. - PubMed
-
- Zellers T.M., Zehr R., Weinstein E., Leonard S., Ring W.S., Nikaidoh H. Two-dimensional and Doppler echocardiography alone can adequately define preoperative anatomy and hemodynamic status before repair of complete atrioventricular septal defect in infants < 1 year old. J Am Coll Cardiol. 1994;24:1565–1570. - PubMed
-
- Benavidez O.J., Gauvreau K., Geva T. Diagnostic errors in congenital echocardiography: importance of study conditions. J Am Soc Echocardiogr. 2014;27:616–623. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
