

Microbiota-derived urolithin A in monoclonal gammopathies and multiple myeloma therapy
- PMID: 40022244
- PMCID: PMC11869585
- DOI: 10.1186/s40168-025-02045-6
Microbiota-derived urolithin A in monoclonal gammopathies and multiple myeloma therapy
Abstract
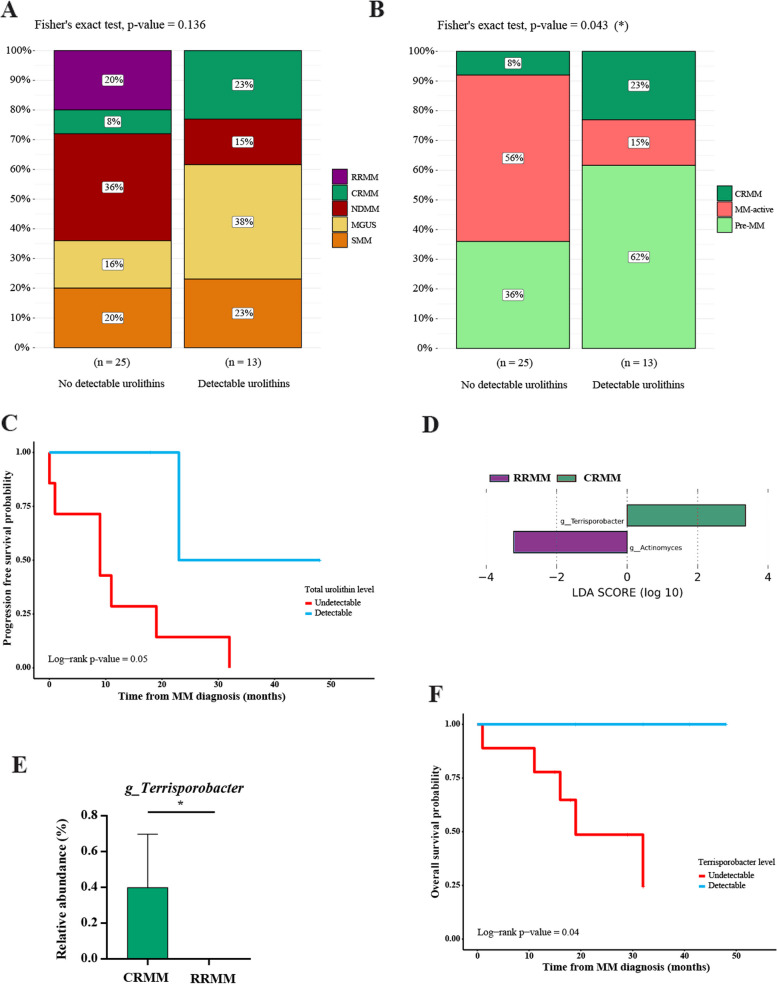
Background: Gut microbiota-derived urolithins may influence multiple myeloma (MM) disease progression and treatment. We analyzed urolithins and their associated microbiota in a retrospective cohort of 45 patients with active MM or premalignant disease using mass spectrometry and 16S rRNA gene sequencing.
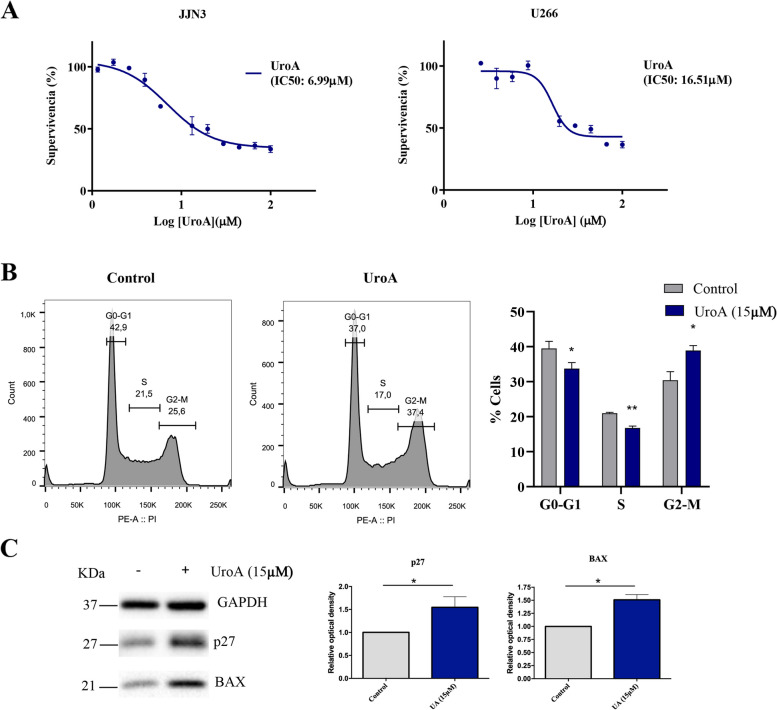
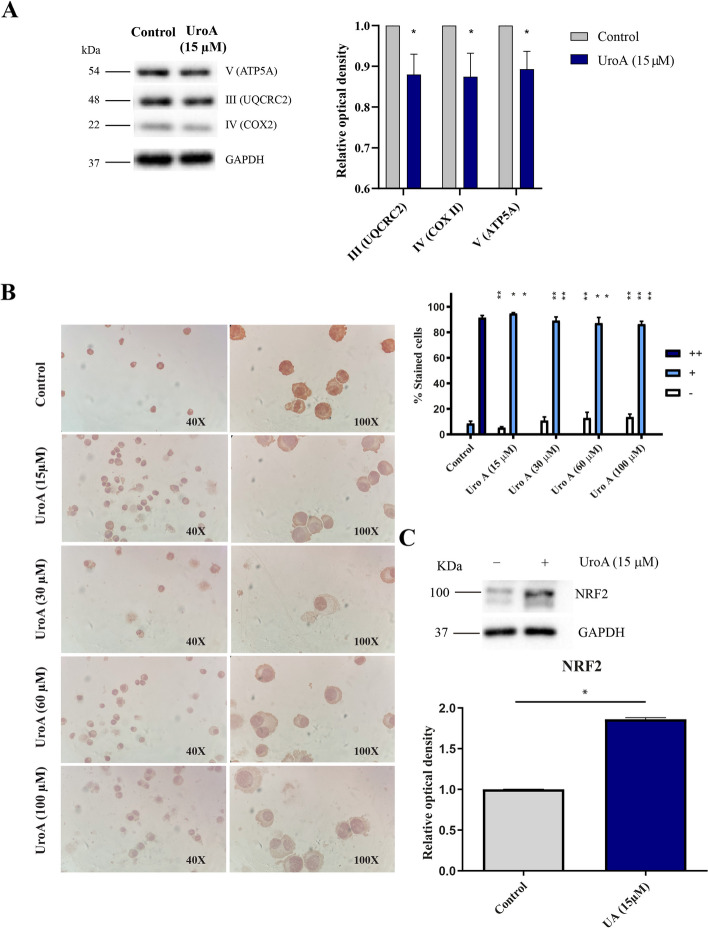
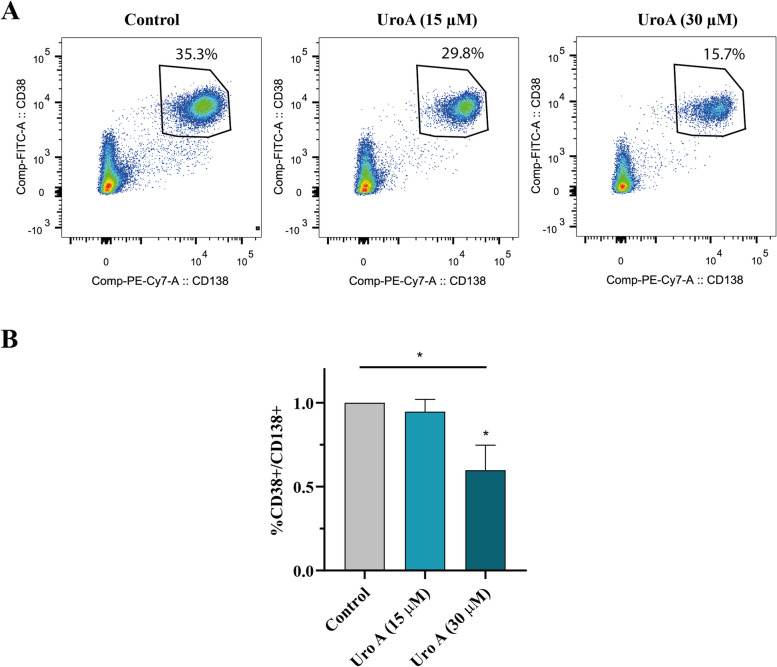
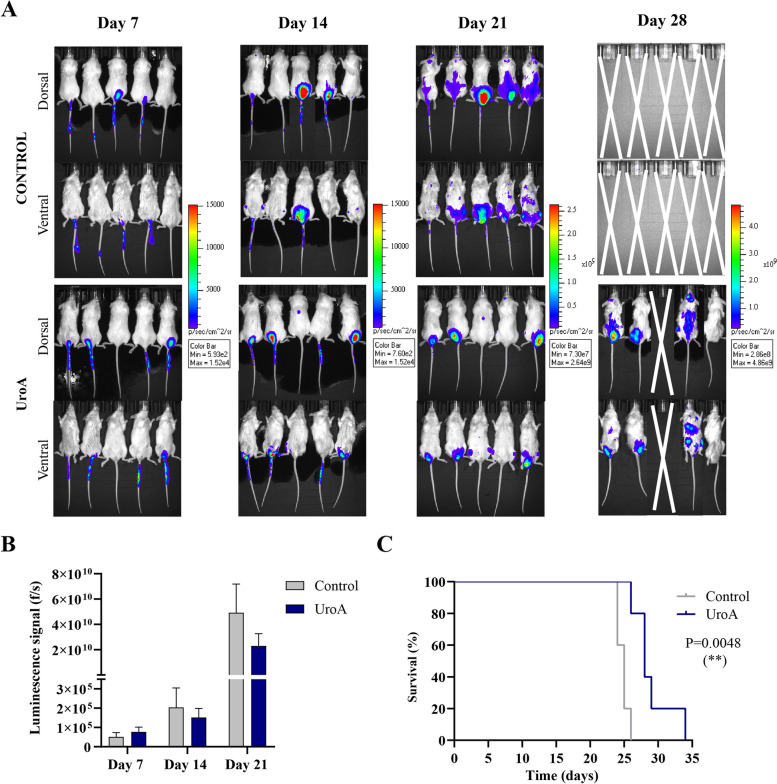
Results: Patients with detectable levels of urolithin in serum and stool and a higher abundance of urolithin-related microbiota had a better outcome. Analysis of the effects of urolithin A (UroA) treatment ex vivo, in vitro, and in vivo revealed that UroA is cytotoxic against MM cell lines and modulates the cell cycle and mitochondrial activity. Notably, UroA inhibits the proliferation of primary MM cells in vitro and in a xenograft mouse model, improving overall survival. Finally, combination therapy with UroA and bortezomib has a synergistic effect in vitro, even in the presence of bortezomib resistance, and modulates signaling pathways involved in MM development.
Conclusions: UroA might be a potential therapeutic agent to halt MM disease progression or to overcome resistance when used in combination. Video Abstract.
Keywords: Gut microbiota; Metabolites; Multiple myeloma; Urolithin.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Hospital 12 de Octubre Ethical Committee (21/580), and all patients and donors provided written informed consent following the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Kyle RA, Remstein ED, Therneau TM, Dispenzieri A, Kurtin PJ, Hodnefield JM, Larson DR, Plevak MF, Jelinek DF, Fonseca R, et al. Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med. 2007;356:2582–90. 10.1056/NEJMoa070389. - PubMed
-
- Bigot-Corbel E, Gassin M, Corre I, Le Carrer D, Delaroche O, Hermouet S. Hepatitis C virus (HCV) infection, monoclonal immunoglobulin specific for HCV core protein, and plasma-cell malignancy. Blood. 2008;112:4357–8. 10.1182/blood-2008-07-167569. - PubMed
-
- Li Y, Li Y, Zhang L, Li W. Hepatitis C virus infection and risk of multiple myeloma: evidence from a meta-analysis based on 17 case-control studies. J Viral Hepat. 2017;24:1151–9. 10.1111/jvh.12742. - PubMed
-
- Yan J, Wang J, Zhang W, Chen M, Chen J, Liu W. Solitary plasmacytoma associated with Epstein-Barr virus: a clinicopathologic, cytogenetic study and literature review. Ann Diagn Pathol. 2017;27:1–6. 10.1016/j.anndiagpath.2016.09.002. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
