

Carbon minibeam radiation therapy results in tumor growth delay in an osteosarcoma murine model
- PMID: 40025099
- PMCID: PMC11873225
- DOI: 10.1038/s41598-025-91872-6
Carbon minibeam radiation therapy results in tumor growth delay in an osteosarcoma murine model
Abstract
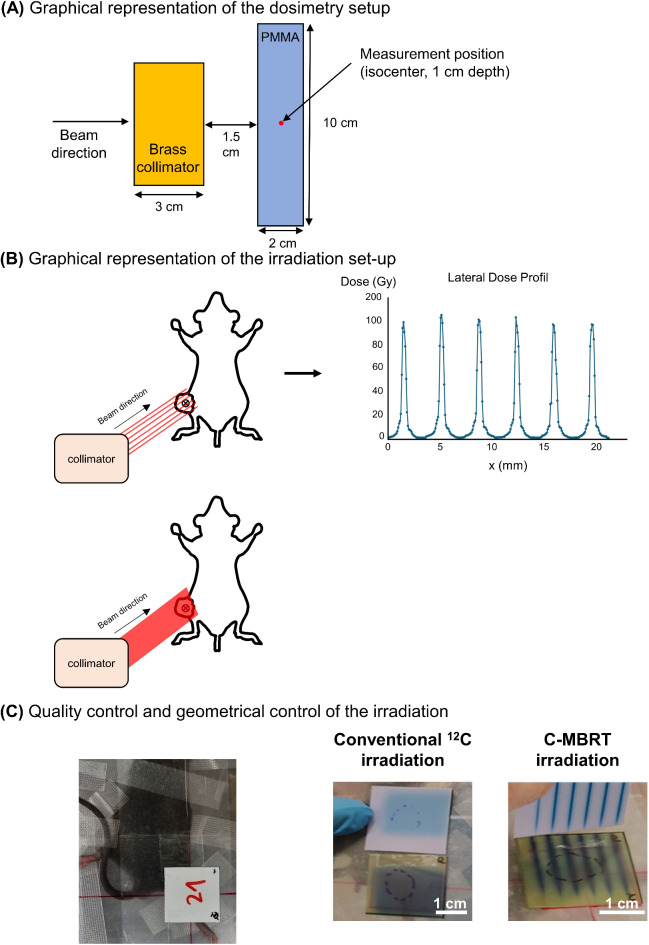
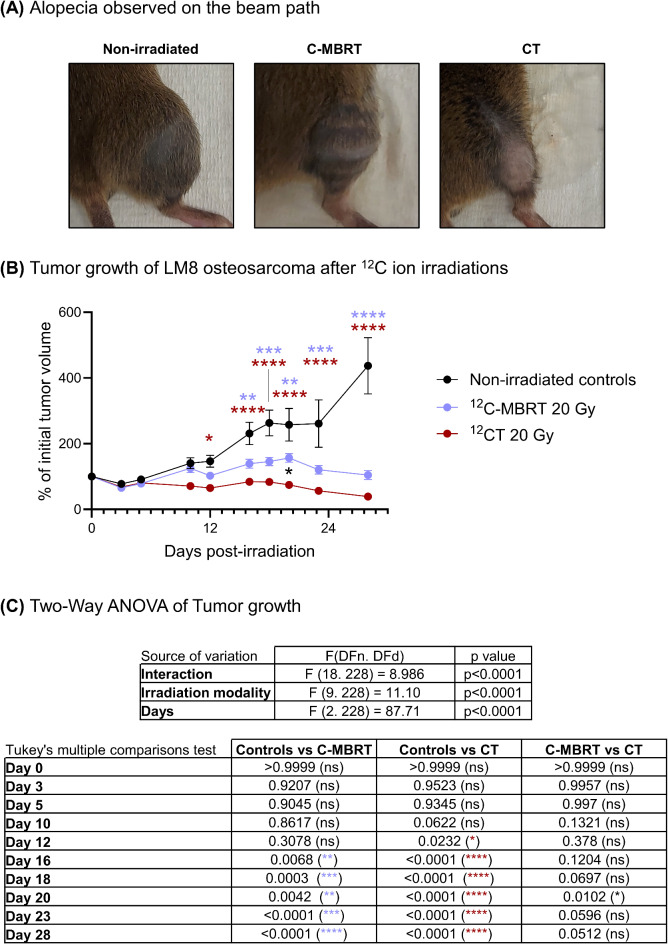
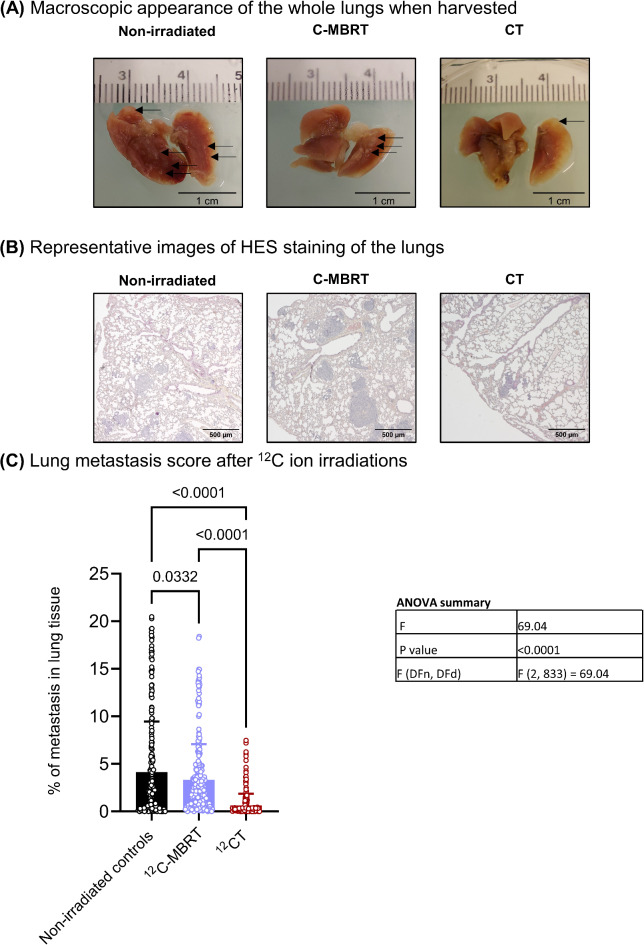
Despite remarkable advances, radiation therapy (RT) remains inefficient for some bulky tumors, radioresistant tumors, and certain pediatric tumors. Minibeam radiation therapy (MBRT) has emerged as a promising approach, reducing normal tissue toxicity while enhancing immune responses. Preclinical studies using X-rays and proton MBRT have demonstrated enhanced therapeutic index for aggressive tumor models. Combining MBRT's advantages of spatial dose fractionation with the physical and biological benefits of carbon ions could be a step further toward unleashing the full potential of MBRT. This study aims to perform the first in vivo study of local and systemic responses of a subcutaneous mouse osteosarcoma (metastatic) model to carbon MBRT (C-MBRT) versus conventional carbon ion therapy (CT). Irradiations were conducted at the GSI Helmholtz Centre in Germany using 180 MeV/u 12C ions beam. All irradiated animals received an average dose (20 Gy) and displayed a significant and similar tumor growth delay in addition to a decreased metastasis score compared to the non-irradiated group. In the C-MBRT group, 70% of the tumor volume received the valley dose, which is a very low dose of 1.5 Gy. The remaining 30% of the tumor received the peak dose of 105 Gy, resulting in an average dose of 20 Gy. These results suggest that C-MBRT triggered distinct mechanisms from CT and encourage further investigations to confirm the potential of C-MBRT for efficient treatment of radioresistant tumors.
Keywords: Carbon ions; Carbon minibeam radiation therapy (C-MBRT); Carbon therapy; Minibeam radiation therapy; Osteosarcoma; Radioresistant tumor.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
-
- Prezado, Y. et al. Spatially fractionated radiation therapy: A critical review on current status of clinical and preclinical studies and knowledge gaps. Phys. Med. Biol.69(10), 1–21, 2024. - PubMed
-
- Deman, P. et al. Monochromatic minibeams radiotherapy: From healthy tissue-sparing effect studies toward first experimental glioma bearing rats therapy. Int. J. Radiat. Oncol. Biol. Phys.82 (4), e693–700 (2012). - PubMed
-
- Prezado, Y. et al. Tolerance to dose escalation in minibeam radiation therapy applied to normal rat brain: Long-term clinical, radiological and histopathological analysis. Radiat. Res.184 (3), 314–321 (2015). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
