

Effects of visual terminal feedback on hand dexterity in relation to visuospatial ability in subacute stroke: a preliminary study
- PMID: 40025159
- PMCID: PMC11873054
- DOI: 10.1038/s41598-025-91806-2
Effects of visual terminal feedback on hand dexterity in relation to visuospatial ability in subacute stroke: a preliminary study
Abstract
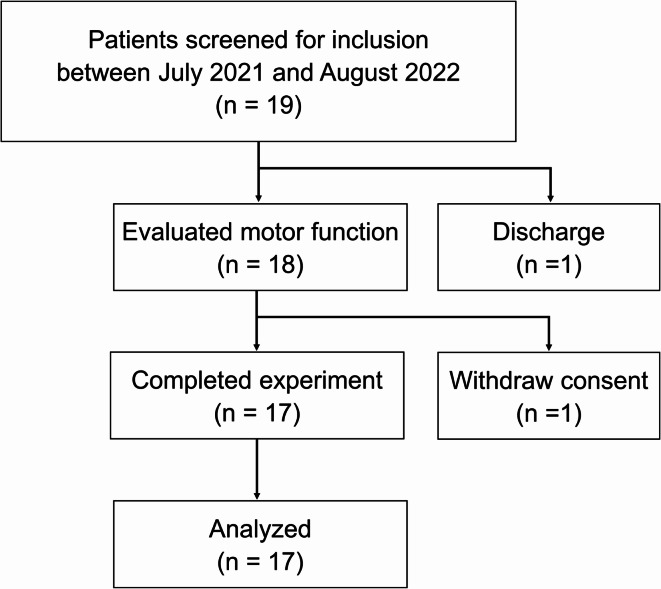
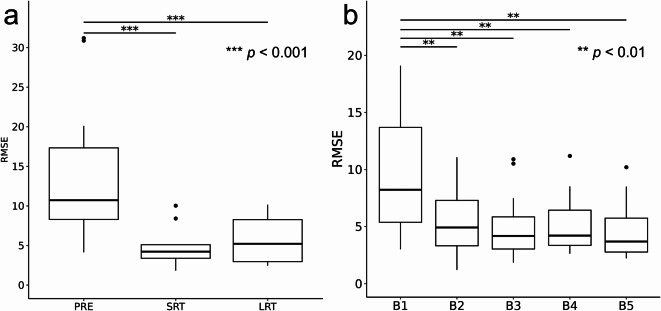
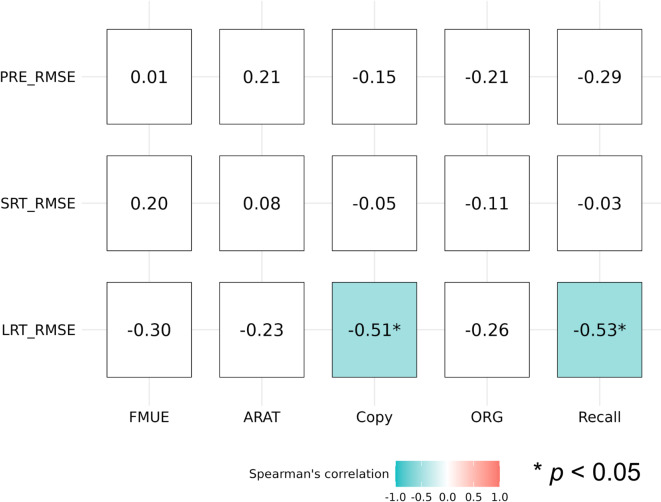
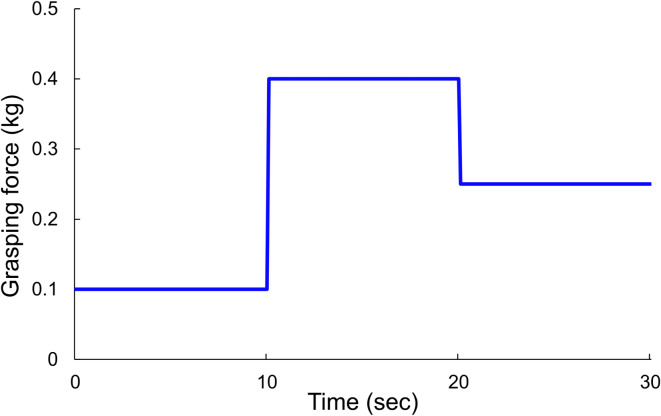
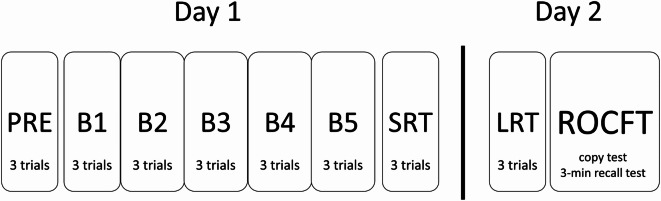
Hand dexterity impairments in patients with stroke reduce activities of daily living (ADL) and quality of life. Visuospatial ability is associated with motor learning, but this has not previously been reported in patients with subacute stroke. We aimed to investigate whether visual terminal feedback (FB) affected motor learning of hand dexterity and the relationship among visuospatial ability. Overall, 17 subacute stroke patients (age: 66.1 ± 13.8 years) with mild upper limb motor impairment were included. The experimental task was the grasping force control task. The visuospatial task was the Rey-Osterrieth Complex Figure Test (ROCFT). The experimental protocol was conducted in 2 consecutive days: day 1 consisted of a pre-test (PRE), practice, and short-term retention test (SRT), and day 2 consisted of a long-term retention test (LRT) and the ROCFT. Grasping errors were significantly decreased in the SRT and LRT than in the PRE. Furthermore, ROCFT scores (copy and recall) and LRT grasping errors were moderately negatively correlated (ρ = -0.51 and - 0.53). In conclusion, visuospatial ability is an important factor associated with motor learning in subacute stroke patients. Future studies should use visual terminal FB, and training programs for visuospatial ability should be considered in stroke rehabilitation.
Keywords: Augmented feedback; Grasping force adjustment ability; Motor learning; Stroke; Task-specific training; Visuospatial ability.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

References
-
- Feigin, V. L. et al. World stroke organization (WSO): global stroke fact sheet 2022. Int. J. Stroke. 17, 18–29 (2022). - PubMed
-
- Birchenall, J. et al. Individual recovery profiles of manual dexterity, and relation to corticospinal lesion load and excitability after stroke –a longitudinal pilot study. Neurophysiol. Clin.49, 149–164 (2019). - PubMed
-
- Pennati, G. V. et al. Recovery and prediction of dynamic precision grip force control after stroke. Stroke.51, 944–951 (2020). - PubMed
-
- Rocha, L. S. O. et al. Constraint induced movement therapy increases functionality and quality of life after stroke. J. Stroke Cerebrovasc. Dis.30, 105774 (2021). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
