

Provision, cough efficacy and treatment satisfaction of mechanical insufflation-exsufflation in a large multicenter cohort of patients with amyotrophic lateral sclerosis
- PMID: 40025240
- PMCID: PMC11873142
- DOI: 10.1038/s41598-025-91692-8
Provision, cough efficacy and treatment satisfaction of mechanical insufflation-exsufflation in a large multicenter cohort of patients with amyotrophic lateral sclerosis
Abstract
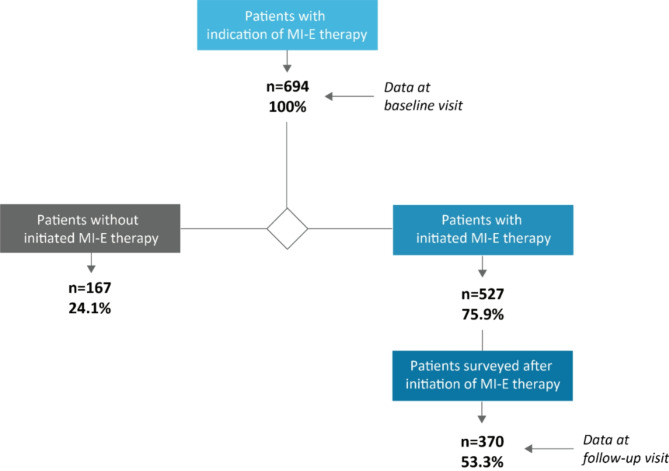
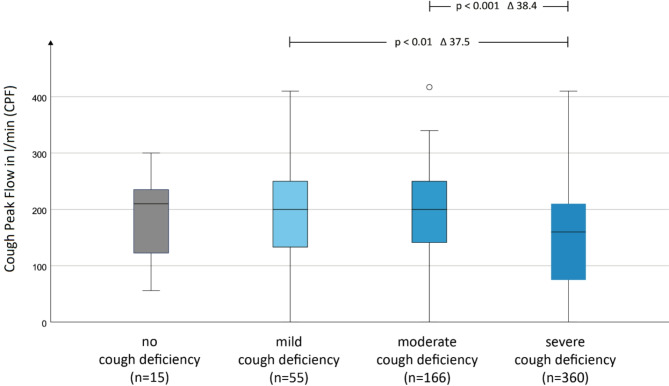
In patients with amyotrophic lateral sclerosis (ALS), mechanical insufflation-exsufflation (MI-E) addresses cough deficiency to achieve major therapeutic goals: improving costal muscle and joint function, reducing atelectasis through insufflation, and clearing bronchial secretions via exsufflation. Despite its perceived benefits, there is limited systematic research on MI-E provision, symptom alleviation, or patient satisfaction. The research platform Ambulanzpartner coordinated this longitudinal observational study conducted in 12 German ALS centers from July 2018 to September 2023. Patients were enrolled based on ALS-related cough deficiency requiring MI-E therapy. The study recorded provision, reasons for withholding MI-E, clinical parameters, therapy frequency, subjective cough deficiency, and symptomatic relief. Satisfaction with MI-E therapy was determined by the likelihood of recommendation. Out of 694 ALS patients indicated for MI-E, 527 (75.9%) received the therapy. The primary reason for non-provision was that the patient had died before provision (n = 66 of 167; 39.5%). These patients were significantly more affected as represented by higher progression rates and lower cough peak flows (CPF) at the time of MI-E indication (p < 0.05). Most patients who received MI-E used it daily (n = 290 of 370; 78.4%). Self-assessed cough deficiency correlated with clinical measurements, especially for patients with higher deficits. At follow-up visits, patients reported reduced cough deficiency (p < 0.001). Frequent MI-E use was linked to greater symptom relief and higher likelihood of recommending the therapy. This study highlights the symptomatic and palliative potential of MI-E therapy for ALS patients.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: AM has received presentation and consulting fees from Merz Pharma GmbH & Co., KGaA, ITF Pharma GmbH, Zambon GmbH and Roche Pharma AG. JCK has received personal fees from AbbVie, Biogen, Ipsen, Roche and Zambon. TM has received consulting fees from Cytokinetics, GSK and Desitin Arzneimittel GmbH, and has served on scientific advisory boards for Cytokinetics, GSK and TEVA. TM and CM are founders of the internet platform Ambulanzpartner and hold shares in Ambulanzpartner Soziotechnologie APST GmbH. SP has participated on advisory boards of Biogen and has received consulting fees from Biogen. AKR received speaker fees from Amylyx Pharmaceuticals and served on advisory boards for Biogen and Argenx outside of the submitted work. All other authors declare that they have no conflicts of interest.
Figures




References
-
- Kiernan, M. C. et al. Amyotrophic lateral sclerosis. Lancet377, 942–955 (2011). - PubMed
-
- Niedermeyer, S., Murn, M. & Choi, P. J. Respiratory failure in amyotrophic lateral sclerosis. Chest155, 401–408 (2019). - PubMed
-
- Tabor-Gray, L., Vasilopoulos, T. & Plowman, E. K. Differences in voluntary and reflexive cough strength in individuals with amyotrophic lateral sclerosis and healthy adults. Muscle Nerve62, 597–600 (2020). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
