

Mechanical chest compression increases intrathoracic hemorrhage complications in patients receiving extracorporeal cardiopulmonary resuscitation
- PMID: 40026714
- PMCID: PMC11870220
- DOI: 10.1016/j.resplu.2025.100892
Mechanical chest compression increases intrathoracic hemorrhage complications in patients receiving extracorporeal cardiopulmonary resuscitation
Abstract
Background: Mechanical cardiopulmonary resuscitation (CPR) devices address the limitations of manual CPR, but their impact on intrathoracic injuries during extracorporeal CPR (ECPR) remains unclear. This study investigated the relationship between mechanical CPR and severe intrathoracic hemorrhage during ECPR compared to manual CPR.
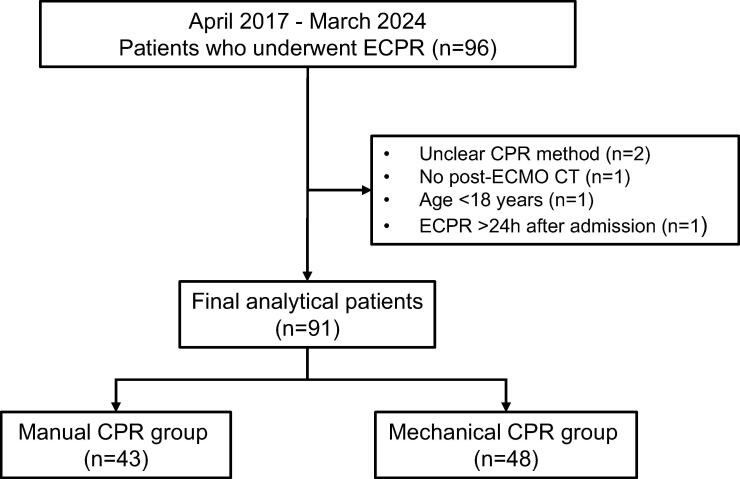
Methods: We conducted a single-center retrospective study of consecutive patients who underwent ECPR from April 2017 to March 2024 according to a standard institutional protocol. Patients were divided into a mechanical CPR group (piston-driven compressions before veno-arterial extracorporeal membrane oxygenation [VA-ECMO]) and a manual CPR group. The primary outcome was intrathoracic hemorrhage requiring transcatheter arterial embolization (TAE). Secondary outcomes included other intrathoracic injuries and 180-day survival.
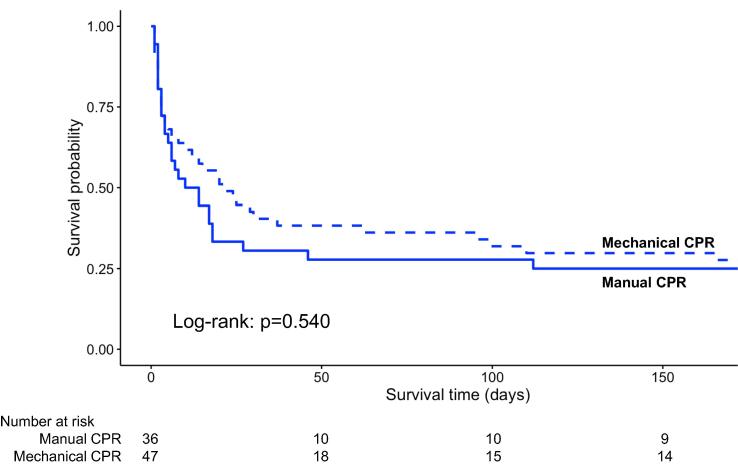
Results: A total of 91 patients were enrolled (mechanical n = 48, manual n = 43). Intrathoracic hemorrhage requiring TAE occurred more frequently in the mechanical CPR group (18.8% vs. 2.3%, p = 0.030). On multivariate analysis, mechanical CPR was independently associated with this outcome (adjusted odds ratio 6.29; 95% confidence interval 1.20-65.10). In the mechanical group, older age and larger thoracic transverse diameter were significantly related to intrathoracic hemorrhage requiring TAE. Mediastinal hematoma (18.8% vs. 2.3%, p = 0.030) and hemothorax (20.8% vs. 4.7%, p = 0.049) were also more frequent in the mechanical group. The 180-day survival rates did not differ significantly between groups (27.7% vs. 25.0%, log-rank p = 0.540).
Conclusions: Mechanical CPR during ECPR is associated with an increased risk of severe intrathoracic hemorrhage. While mechanical CPR devices may provide benefits in certain scenarios, clinicians should carefully consider individual patient characteristics and closely monitor for complications.
Keywords: Cardiopulmonary resuscitation; Chest compression; Extracorporeal cardiopulmonary resuscitation; Intrathoracic hemorrhage; Mechanical chest compression device; Thoracic injury.
© 2025 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Outcomes after mechanical versus manual chest compressions in eCPR patients.Expert Rev Med Devices. 2021 Oct;18(10):1023-1028. doi: 10.1080/17434440.2021.1970528. Epub 2021 Aug 27. Expert Rev Med Devices. 2021. PMID: 34424111
-
Mechanical versus manual chest compressions for cardiac arrest.Cochrane Database Syst Rev. 2018 Aug 20;8(8):CD007260. doi: 10.1002/14651858.CD007260.pub4. Cochrane Database Syst Rev. 2018. PMID: 30125048 Free PMC article.
-
Time to initiation of extracorporeal membrane oxygenation in conventional cardiopulmonary resuscitation affects the patient survival prognosis.J Intern Med. 2024 Oct;296(4):350-361. doi: 10.1111/joim.20002. Epub 2024 Jul 29. J Intern Med. 2024. PMID: 39073177
-
Compression Device-Assisted Extracorporeal Cardiopulmonary Resuscitation Cannulation in Pediatric Patients-A Simulation Study.World J Pediatr Congenit Heart Surg. 2022 May;13(3):379-382. doi: 10.1177/21501351221084304. World J Pediatr Congenit Heart Surg. 2022. PMID: 35446221
-
Extracorporeal Membrane Oxygenation for Cardiac Indications in Adults: A Health Technology Assessment.Ont Health Technol Assess Ser. 2020 Mar 6;20(8):1-121. eCollection 2020. Ont Health Technol Assess Ser. 2020. PMID: 32284771 Free PMC article.
References
-
- Panchal A.R., Bartos J.A., Cabañas J.G., et al. Part 3: Adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142:S366–S468. - PubMed
-
- Idris A.H., Guffey D., Pepe P.E., et al. Chest compression rates and survival following out-of-hospital cardiac arrest. Crit Care Med. 2015;43:840–848. - PubMed
-
- McDonald C.H., Heggie J., Jones C.M., Thorne C.J., Hulme J. Rescuer fatigue under the 2010 ERC guidelines, and its effect on cardiopulmonary resuscitation (CPR) performance. Emerg Med J. 2013;30:623–627. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
