

Weight gain among children under five with severe malnutrition in therapeutic feeding programmes: a systematic review and meta-analysis
- PMID: 40026833
- PMCID: PMC11872456
- DOI: 10.1016/j.eclinm.2025.103083
Weight gain among children under five with severe malnutrition in therapeutic feeding programmes: a systematic review and meta-analysis
Abstract
Background: Globally, some 45 million children under five years of age are wasted (low weight-for-height). Although 2023 World Health Organisation guidelines on their care did not aim to identify optimal weight gain, they did mention 5-10 g/kg/day as a target, which is a change from prior guidelines that recommended 10-15 g/kg/day, when inpatient-only care was the norm. We aimed to inform future policy/programming on weight gain targets.
Methods: For this systematic review and meta-analysis, we searched Embase, Global Health and Medline. The final search was on 23/02/2024. Papers were included if they reported weight gain of children aged 6-59 months with severe malnutrition during inpatient (facility-based), outpatient (home-based), and hybrid treatment (initially inpatient and progressing to outpatient treatment). Summary data were extracted, and quality was assessed using a NICE Quality Appraisal Checklist. Our primary outcome was mean rate of weight gain (g/kg/day) during treatment. We conducted random-effects meta-analysis to describe pooled mean weight gain by programme type. Meta-regression investigated potential associations of weight gain with length of stay and programme outcomes. We registered the study on PROSPERO (CRD42023266472).
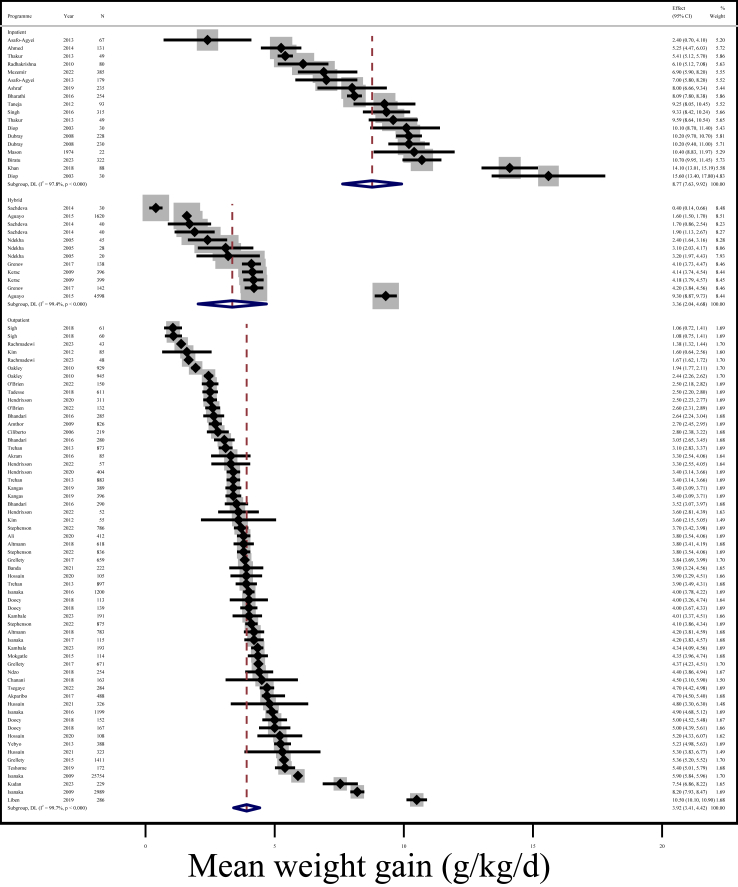
Findings: Our search yielded 3173 papers. We reviewed 321 full texts, identifying 126 eligible papers. Of these, 104 papers, including some 240,650 participants, reported weight gain as g/kg/day and were eligible for meta-analysis. Mean rate of weight gain was 8.8 g/kg/day (95% CI: 7.6, 9.9; I2 = 97.8%) across 18 inpatient programmes, 3.4 g/kg/day (95% CI: 2.0, 4.7; I2 = 99.4%) across 12 hybrid programmes, and 3.9 g/kg/day (95% CI: 3.4, 4.4; I2 = 99.7%) across 60 outpatient programmes. We found inconsistent evidence of an association between slower weight gain and higher mortality: there was weak evidence of association after adjusting for programme type (coefficient = -0.4; 95% CI: -0.7, -0.02; p = 0.04; n = 118 programmes). There was high heterogeneity between studies. Details of weight gain calculation methods varied. We found no evidence for publication bias when accounting for programme type (Egger's test p-value = 0.2).
Interpretation: Weight gain in outpatient programmes was markedly slower than in inpatient treatment. Clearer reporting of weight gain and a better understanding of the sequelae of faster/slower recovery is important to set future weight gain targets. Our results set an important baseline for current programmes to benchmark against.
Funding: Medical Research Council/Global Challenges Research Fund, grant number: MR/V000802/1.
Keywords: Catch-up growth; Child health; Severe malnutrition; Therapeutic feeding programmes; Weight gain.
© 2025 The Authors.
Conflict of interest statement
DT received WHO funding to attend two WHO Guideline Development Group meetings. We have no other competing interests to declare.
Figures



References
-
- UNICEF/WHO/World Bank Child malnutrition - UNICEF data. 2023. https://data.unicef.org/topic/nutrition/malnutrition
-
- Black R.E., Victora C.G., Walker S.P., et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–451. - PubMed
-
- World Health Organization, UNICEF . World Health Organizartion; Geneva: 2009. WHO Child Growth Standards and the Identification of Severe Acute Malnutrition in Infants and Children: A Joint Statement by the World Health Organization and the United Nation’s Children Fund. - PubMed
-
- Frison S., Checchi F., Kerac M. Omitting edema measurement: how much acute malnutrition are we missing? Am J Clin Nutr. 2015;102(5):1176–1181. - PubMed
LinkOut - more resources
Full Text Sources
