

Predictive validity of the sequential organ failure assessment score for mortality in patients with acute respiratory distress syndrome in Vietnam
- PMID: 40033012
- PMCID: PMC11876689
- DOI: 10.1038/s41598-025-92199-y
Predictive validity of the sequential organ failure assessment score for mortality in patients with acute respiratory distress syndrome in Vietnam
Abstract
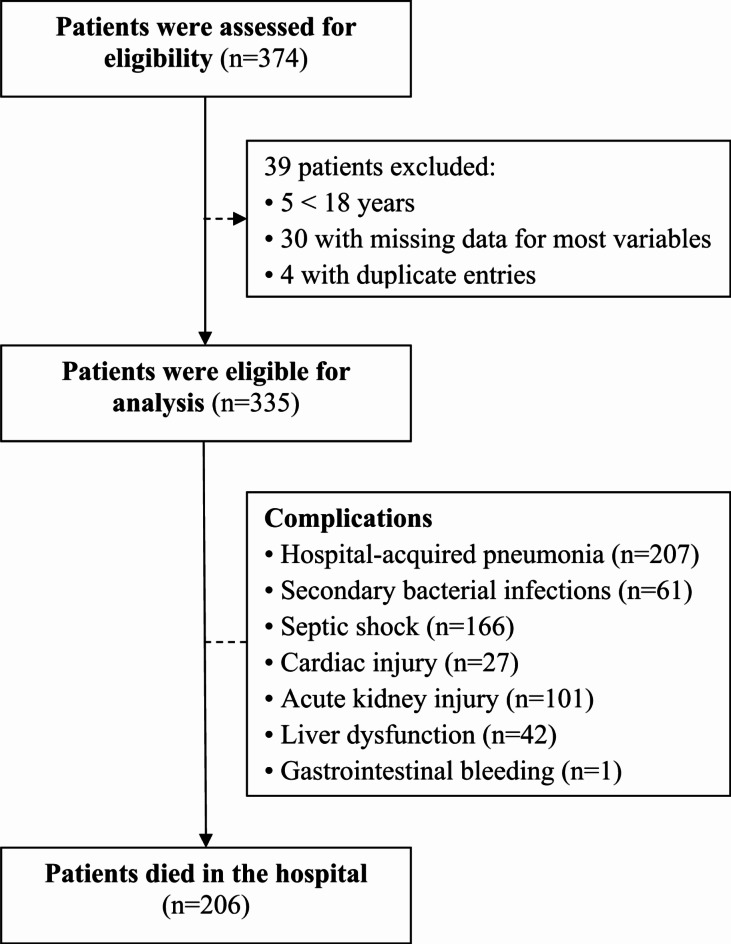
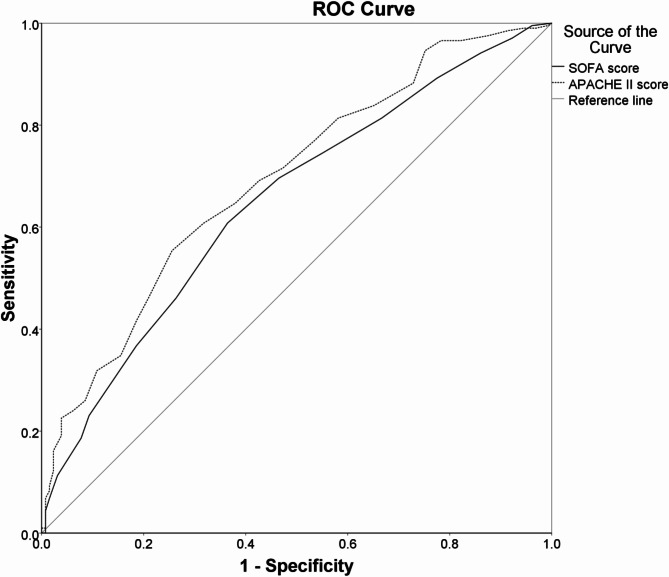
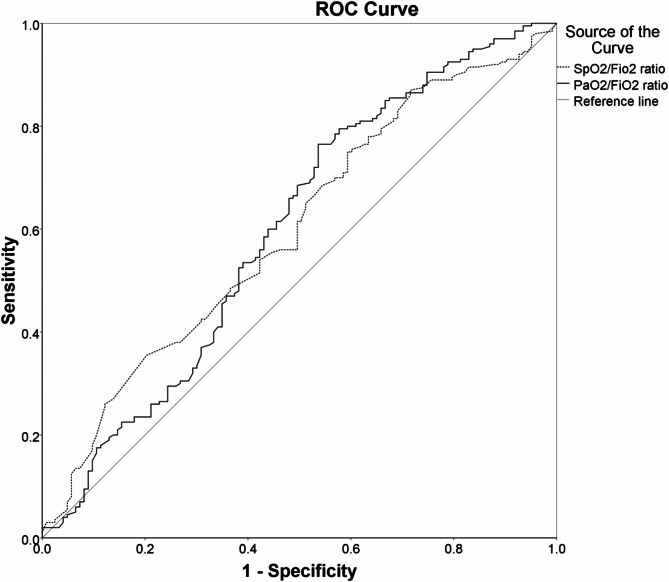
Evaluating the prognosis of ARDS patients using grading systems can enhance treatment decisions. This retrospective observational study evaluated the predictive accuracy of the SOFA score, APACHE II score, SpO2/FiO2 ratio, and PaO2/FiO2 ratio for mortality in ARDS patients in Vietnam. The study included 335 adult ARDS patients admitted to a central hospital from August 2015 to August 2023. Among them, 66.9% were male, the median age was 55 years, and 61.5% died in the hospital. The SOFA (AUROC: 0.651) and APACHE II scores (AUROC: 0.693) showed poor discriminatory ability for hospital mortality. The SpO2/FiO2 (AUROC: 0.595) and PaO2/FiO2 ratios (AUROC: 0.595) also displayed poor discriminatory ability. In multivariable analyses, after adjusting for the same set of confounding variables, the APACHE II score (adjusted OR: 1.152), SpO2/FiO2 ratio (adjusted OR: 0.985), and PaO2/FiO2 ratio (adjusted OR: 0.989) were independently associated with hospital mortality. Although the SOFA score (adjusted OR: 1.132) indicated a potential association with hospital mortality, it did not reach statistical significance (p = 0.081). However, a SOFA score of ≥ 10 emerged as an independent predictor (adjusted OR: 3.398) of hospital mortality. These findings emphasize the need for further studies to develop more accurate scoring systems for predicting outcomes in ARDS patients.
Keywords: APACHE II score; Acute respiratory distress syndrome (ARDS); Berlin definition criteria; Critical care; Mechanical ventilation; Mortality; New global definition; PaO2/FiO2 ratio; SOFA score; SpO2/FiO2 ratio.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Consent for publication: Not applicable.
Figures
References
-
- Peter, J. V. et al. Corticosteroids in the prevention and treatment of acute respiratory distress syndrome (ARDS) in adults: meta-analysis. Bmj336, 1006–1009. 10.1136/bmj.39537.939039.BE (2008). - PMC - PubMed
-
- Bellani, G. et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. Jama315, 788–800. 10.1001/jama.2016.0291 (2016). - PubMed
-
- Stapleton, R. D. et al. Causes and timing of death in patients with ARDS. Chest128, 525–532. 10.1378/chest.128.2.525 (2005). - PubMed
-
- Montgomery, A. B., Stager, M. A., Carrico, C. J. & Hudson, L. D. Causes of mortality in patients with the adult respiratory distress syndrome. Am. Rev. Respir. Dis.132, 485–489. 10.1164/arrd.1985.132.3.485 (1985). - PubMed
-
- Bersten, A. D., Edibam, C., Hunt, T. & Moran, J. Incidence and mortality of acute lung injury and the acute respiratory distress syndrome in three Australian States. Am. J. Respir. Crit Care Med.165, 443–448. 10.1164/ajrccm.165.4.2101124 (2002). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
