

Explainable machine learning model for predicting acute pancreatitis mortality in the intensive care unit
- PMID: 40033198
- PMCID: PMC11877909
- DOI: 10.1186/s12876-025-03723-3
Explainable machine learning model for predicting acute pancreatitis mortality in the intensive care unit
Abstract
Background: Current prediction models are suboptimal for determining mortality risk in patients with acute pancreatitis (AP); this might be improved by using a machine learning (ML) model. In this study, we aimed to construct an explainable ML model to calculate the risk of mortality in patients with AP admitted in intensive care unit (ICU) and compared it with existing scoring systems.
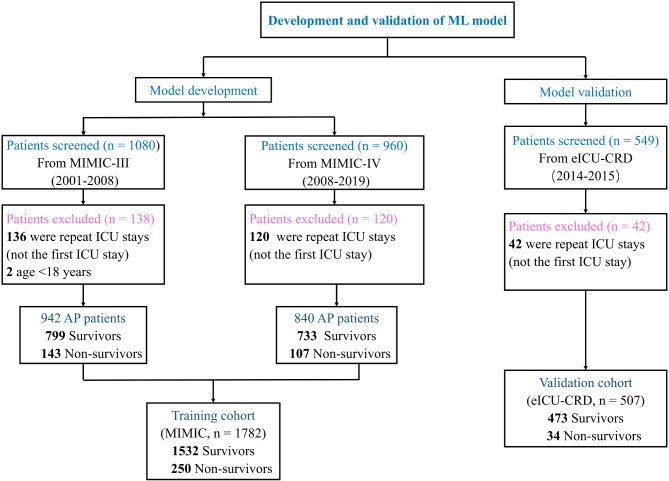
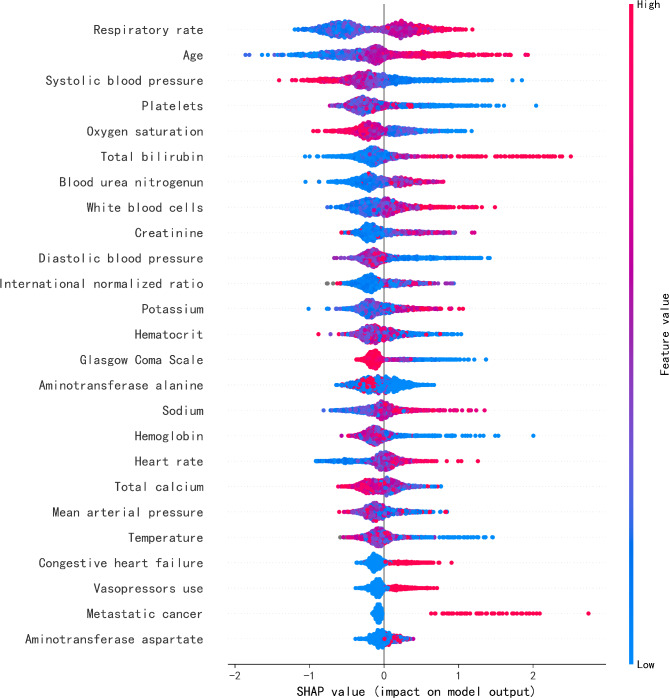
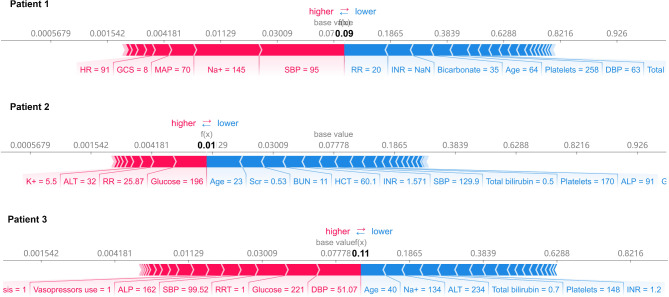
Methods: A gradient-boosting ML (XGBoost) model was developed and externally validated based on two public databases: Medical Information Mart for Intensive Care (MIMIC, training cohort) and the eICU Collaborative Research Database (eICU-CRD, validation cohort). We compared the performance of the XGBoost model with validated clinical risk scoring systems (the APACHE IV, SOFA, and Bedside Index for Severity in Acute Pancreatitis [BISAP]) by area under receiver operating characteristic curve (AUC) analysis. SHAP (SHapley Additive exPlanations) method was applied to provide the explanation behind the prediction outcome.
Results: The XGBoost model performed better than the clinical scoring systems in correctly predicting mortality risk of AP patients, achieving an AUC of 0.89 (95% CI: 0.84-0.94). When set the sensitivity at 100% for death prediction, the model had a specificity of 38%, much higher than the APACHE IV, SOFA and BISAP score, which had a specificity of 1%, 16% and 1% respectively.
Conclusions: This model might increase identification of very low-risk patients who can be safely monitored in a general ward for management. By making the model explainable, physicians would be able to better understand the reasoning behind the prediction.
Keywords: Acute pancreatitis; Mortality; Prediction; Prognostic factor; XGBoost.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Since the study was an analysis of the third party anonymized publicly available database with pre-existing institutional review board (IRB) approval, IRB approval from The First Affiliated Hospital of Zhejiang university was waived. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Boxhoorn L, Voermans RP, Bouwense SA, Bruno MJ, Verdonk RC, Boermeester MA, et al. Acute pancreatitis. Lancet. 2020;396(10252):726–34. - PubMed
-
- Buter A, Imrie CW, Carter CR, Evans S, McKay CJ. Dynamic nature of early organ dysfunction determines outcome in acute pancreatitis. Brit J Surg. 2002;89(3):298–302. - PubMed
-
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–11. - PubMed
-
- Di MY, Liu H, Yang ZY, Bonis PA, Tang JL, Lau J. Prediction models of mortality in acute pancreatitis in adults: A systematic review. Ann Intern Med. 2016;165(7):482–90. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
