

Tension pneumothorax from large bowel herniation and perforation as a late presentation of traumatic diaphragmatic hernia during pregnancy: a case report
- PMID: 40033229
- PMCID: PMC11874637
- DOI: 10.1186/s12245-025-00843-1
Tension pneumothorax from large bowel herniation and perforation as a late presentation of traumatic diaphragmatic hernia during pregnancy: a case report
Abstract
Background: Diaphragmatic hernias can be congenital or acquired, with trauma being the primary cause of the latter. Both types may have delayed presentations, with abdominal organs protruding into the thoracic cavity, causing symptoms of varying severity. Pregnancy can sometimes precipitate the condition. Tension pneumothorax resulting from bowel perforation into the thorax is exceptionally rare, with only a few cases reported. To the best of the authors knowledge, this is the third documented case of a late-presenting trauma-related diaphragmatic hernia during pregnancy, complicated by tension pneumothorax.
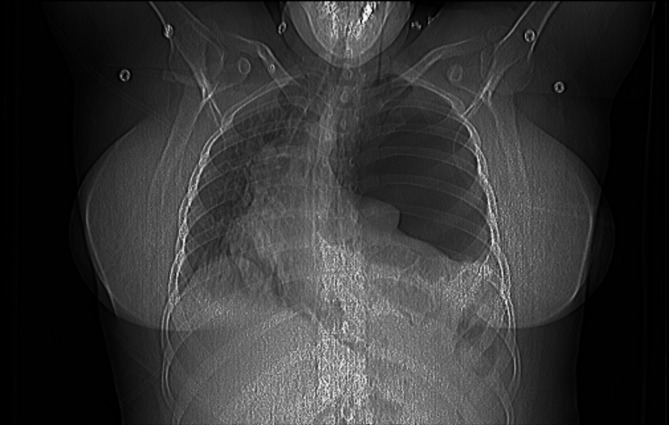
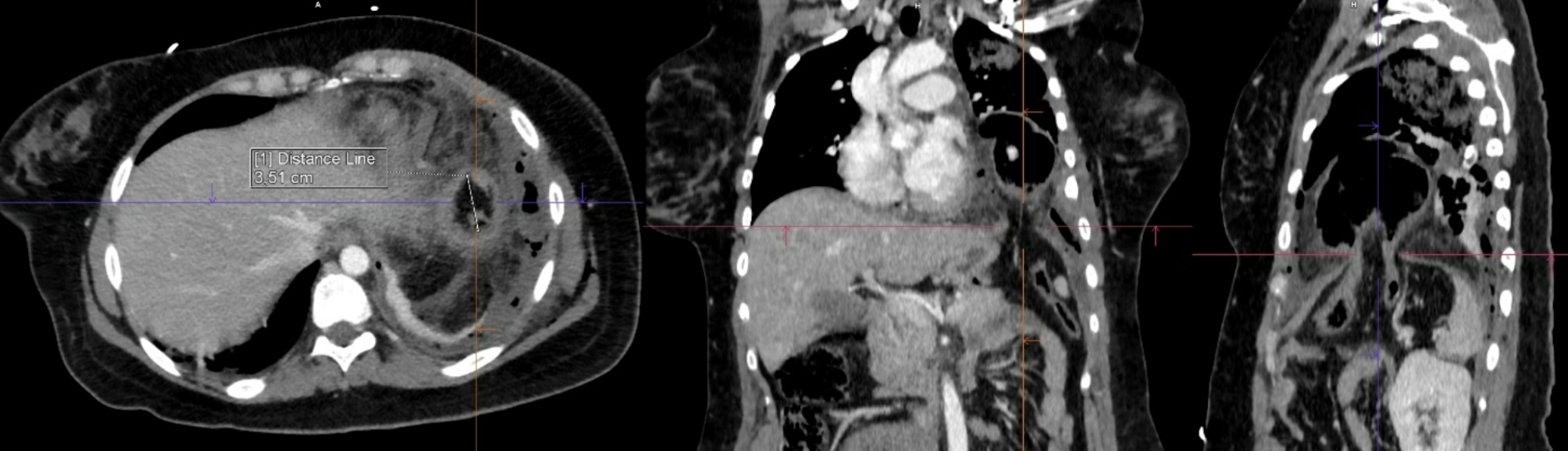
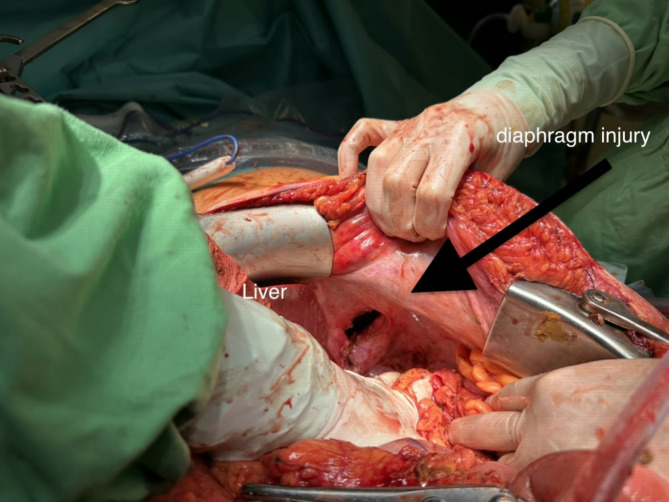
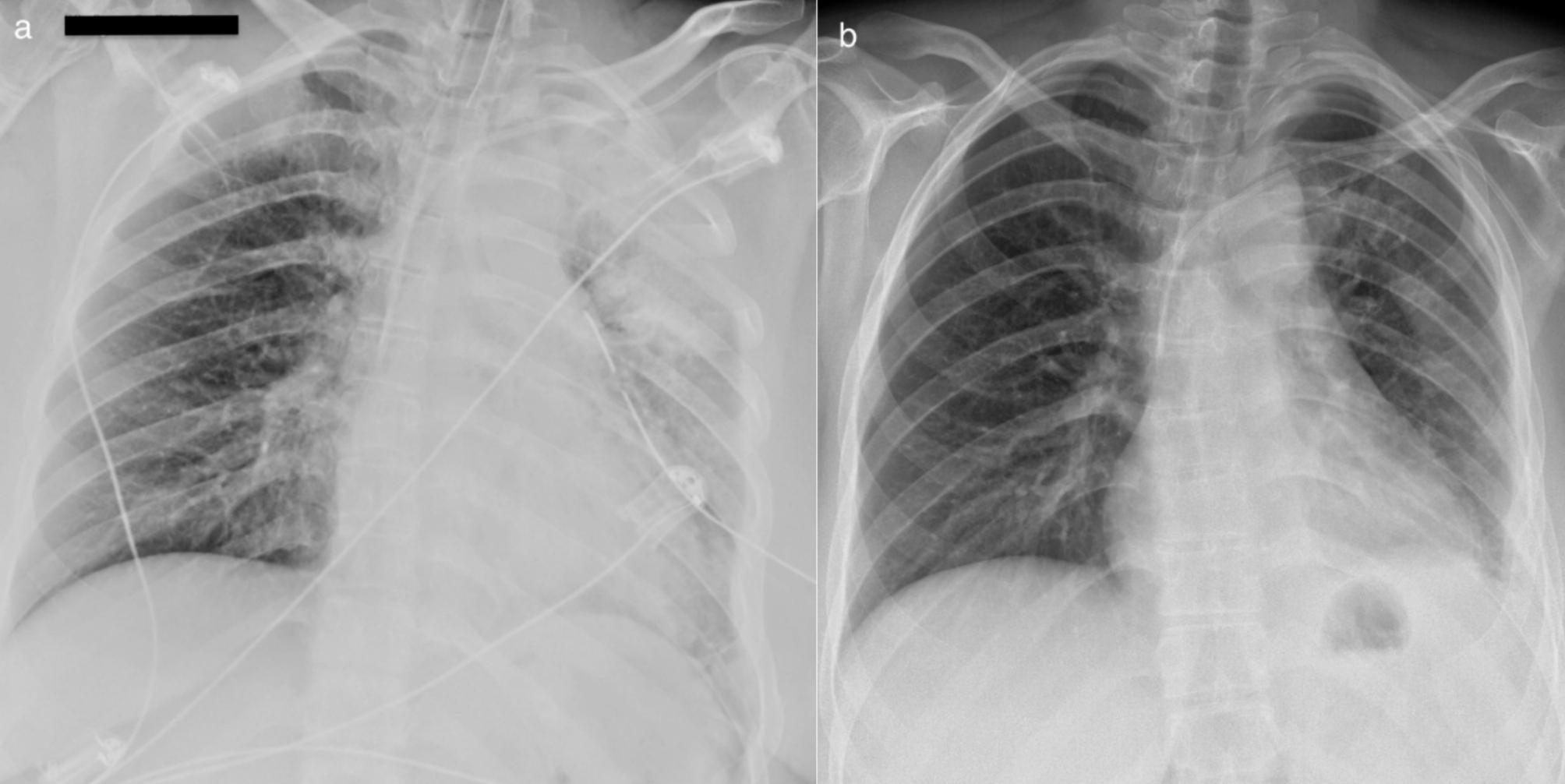
Case presentation: A 30-year-old woman, 29 weeks pregnant, was referred to Semmelweis University emergency department with moderate dyspnea. Initial investigation revealed tension pneumothorax. Chest tube placement released air, pus, and feces. Computer tomography identified a diaphragmatic hernia with bowel incarceration and perforation as the underlying cause. The patient underwent a delayed cesarean section and surgical repair, with a good outcome. A history of thoracic trauma eight years prior was later revealed.
Conclusion: Evaluating pregnant patients with shortness of breath in the emergency department is challenging. Identifying a history of thoracic or abdominal trauma is crucial, as this can raise the suspicion of diaphragmatic hernia, which can present with a wide range of symptoms. Spontaneous tension pneumothorax in pregnant women is extremely rare and requires cautious management. A multidisciplinary approach is crucial for the successful treatment of maternal diaphragmatic hernia.
Keywords: Diaphragmatic hernia; Dyspnea; Empyema; Large bowel perforation; Pregnancy; Tension pneumothorax.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Written informed consent was obtained from the patient for publication of this case report and accompanying images. Competing interests: The authors declare no competing interests.
Figures



References
-
- Mullins ME, Stein J, Saini SS, Mueller PR. Prevalence of incidental Bochdalek’s hernia in a large adult population. AJR Am J Roentgenol. 2001;177(2):363–6. - PubMed
-
- Brown SR, Horton JD, Trivette E, Hofmann LJ, Johnson JM. Bochdalek hernia in the adult: demographics, presentation, and surgical management. Hernia. 2011;15(1):23–30. - PubMed
-
- Cusumano C, Kansoun A, Kamga Tougoue F, de Mathelin P, Bachellier P, Addeo P. Incidence and outcomes of post-hepatectomy diaphragmatic hernia: a systematic review. HPB (Oxford). 2023;25(12):1466–74. - PubMed
-
- Fair KA, Gordon NT, Barbosa RR, Rowell SE, Watters JM, Schreiber MA. Traumatic diaphragmatic injury in the American College of Surgeons National Trauma Data Bank: a new examination of a rare diagnosis. Am J Surg. 2015;209(5):864-8; discussion 8–9. - PubMed
LinkOut - more resources
Full Text Sources
