

Joint association of remnant cholesterol and lipoprotein-associated phospholipase A2 with composite adverse events: A 12-year follow-up study from Asymptomatic Polyvascular Abnormalities Community study
- PMID: 40035211
- PMCID: PMC11964985
- DOI: 10.1111/dom.16286
Joint association of remnant cholesterol and lipoprotein-associated phospholipase A2 with composite adverse events: A 12-year follow-up study from Asymptomatic Polyvascular Abnormalities Community study
Abstract
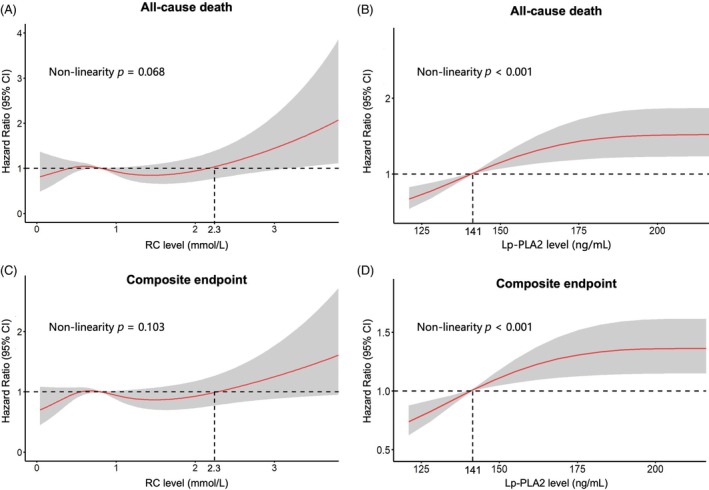
Aims: To explore the association of remnant cholesterol (RC) and lipoprotein-associated phospholipase A2 (Lp-PLA2) with composite adverse events in a large-scale prospective study.
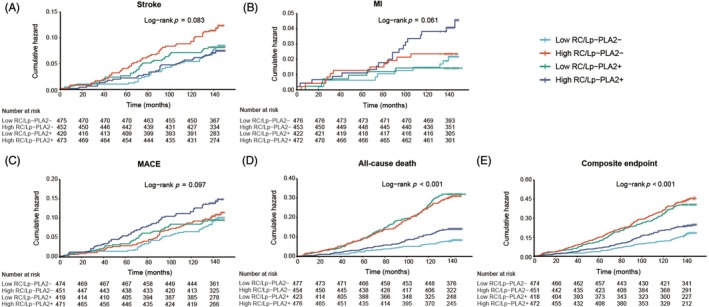
Methods: All data were collected from the Asymptomatic Polyvascular Abnormalities Community study between 2010 and 2022. Serum cholesterol levels and Lp-PLA2 were determined by enzyme-linked immunosorbent assay. The participants were categorized into four groups based on their RC and Lp-PLA2 levels: low-RC/Lp-PLA2-, high-RC/Lp-PLA2-, low-RC/Lp-PLA2+ and high-RC/Lp-PLA2+. The composite endpoint was a combination of first-ever stroke, myocardial infarction or all-cause mortality. Cox regression analyses were performed to evaluate associations of RC and Lp-PLA2 with composite adverse events.
Results: Of the 1864 eligible participants, the average age was 60.6 years, and 74.3% were male. Over a follow-up of 12 years, we identified 500 composite adverse events, including 210 major adverse cardiovascular events and 342 all-cause deaths. When compared with the group of low-RC/Lp-PLA2-, the hazard ratios with 95% confidence intervals in the group of high-RC/Lp-PLA2+ for stroke, myocardial infarction, major adverse cardiovascular event, all-cause death and composite endpoints were 1.37 (0.87-2.16), 0.72 (0.28-1.82), 1.29 (0.85-1.95), 1.61 (1.10-2.38) and 1.43 (1.07-1.91), respectively. A significant interaction between RC and Lp-PLA2 status has been found for all-cause death and composite endpoint (p for interaction <0.05). In addition, joint association of RC and Lp-PLA2 with all-cause death was modified by sex and age of <60 versus ≥60 years (p for interaction: 0.035 and 0.01, respectively).
Conclusions: Elevated RC and Lp-PLA2 levels were associated with an increased risk of composite adverse events, with these associations significantly influenced by sex and age. Our study highlights the synergistic effect of RC and Lp-PLA2 on the composite adverse events.
Keywords: lipoprotein‐associated phospholipase A2; prospective study; remnant cholesterol.
© 2025 The Author(s). Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no competing financial/non‐financial interests.
Figures
Similar articles
-
The Use of Lipoprotein-Associated Phospholipase A2 in a Chinese Population to Predict Cardiovascular Events.Biomed Environ Sci. 2022 Mar 20;35(3):206-214. doi: 10.3967/bes2022.029. Biomed Environ Sci. 2022. PMID: 35317900
-
Elevated Lp-PLA2 levels add prognostic information to the metabolic syndrome on incidence of cardiovascular events among middle-aged nondiabetic subjects.Arterioscler Thromb Vasc Biol. 2007 Jun;27(6):1411-6. doi: 10.1161/ATVBAHA.107.142679. Epub 2007 Apr 12. Arterioscler Thromb Vasc Biol. 2007. PMID: 17431184
-
Prognostic value of lipoprotein-associated phospholipase A2 mass for all-cause mortality and vascular events within one year after acute ischemic stroke.Atherosclerosis. 2017 Nov;266:1-7. doi: 10.1016/j.atherosclerosis.2017.09.013. Epub 2017 Sep 14. Atherosclerosis. 2017. PMID: 28934604
-
The role of lipoprotein-associated phospholipase A2 in atherosclerosis may depend on its lipoprotein carrier in plasma.Biochim Biophys Acta. 2009 May;1791(5):327-38. doi: 10.1016/j.bbalip.2009.02.015. Biochim Biophys Acta. 2009. PMID: 19272461 Review.
-
[Lipoprotein-associated phospholipase A(2) and stroke].Rev Neurol. 2009 Jul 16-31;49(2):88-94. Rev Neurol. 2009. PMID: 19598138 Review. Spanish.
References
-
- Sasso FC, Lascar N, Ascione A, et al. Moderate‐intensity statin therapy seems ineffective in primary cardiovascular prevention in patients with type 2 diabetes complicated by nephropathy. A multicenter prospective 8 years follow up study. Cardiovasc Diabetol. 2016;15(1):147. doi:10.1186/s12933-016-0463-9 - DOI - PMC - PubMed
-
- Nambi V, Hoogeveen RC, Chambless L, et al. Lipoprotein‐associated phospholipase A2 and high‐sensitivity C‐reactive protein improve the stratification of ischemic stroke risk in the atherosclerosis risk in communities (ARIC) study. Stroke. 2009;40(2):376‐381. doi:10.1161/STROKEAHA.107.513259 - DOI - PMC - PubMed
-
- Oei H‐HS, van der Meer IM, Hofman A, et al. Lipoprotein‐associated phospholipase A2 activity is associated with risk of coronary heart disease and ischemic stroke: the Rotterdam study. Circulation. 2005;111(5):570‐575. doi:10.1161/01.CIR.0000154553.12214.CD - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
