

Neonatal enlargement of the aortic arch roof without cardiopulmonary bypass using ductal patency for lower body perfusion: impact on long-term growth, function and shape of the aortic arch†
- PMID: 40036316
- PMCID: PMC11997790
- DOI: 10.1093/icvts/ivaf042
Neonatal enlargement of the aortic arch roof without cardiopulmonary bypass using ductal patency for lower body perfusion: impact on long-term growth, function and shape of the aortic arch†
Abstract
Objectives: This study evaluates the long-term outcome of neonatal aortic arch roof enlargement using ductal patency in the context of coarctation associated with aortic arch hypoplasia.
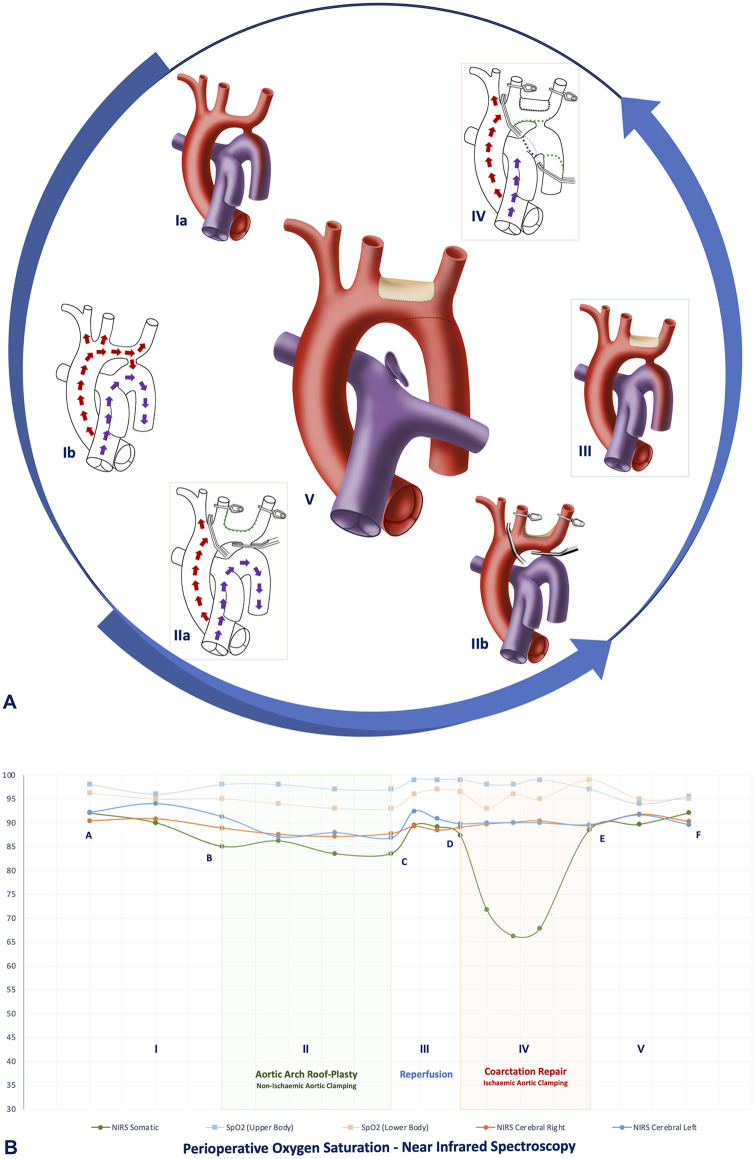
Methods: Retrospective single-centre analysis of children undergoing roof enlargement of the distal arch (left common carotid artery-left subclavian artery) without cardiopulmonary bypass (utilizing ductal patency for lower body perfusion); followed by resection and extended end-to-end anastomosis, through a left posterior thoracotomy. This study evaluates the long-term outcome with emphasis on arch growth and shape.
Results: Thirty consecutive patients were included (2006-24). Median age and weight were 6.0 [interquartile range: 4.0-7.8)] days and 3.1 (2.7-3.5) kg, respectively. Simple congenital heart disease with simple intracardiac shunts (n = 17) and complex congenital heart disease (Complete Atrioventricular Septal Defect (AVSD), interrupted aortic arch and univentricular hearts) (n = 13) constituted the cohort. Non-ischaemic clamp time for roof enlargement was 43 (36-50) min. Ischaemic clamp time for coarctation resection was 23 (21-25) min. Pulmonary artery banding was performed in 19 (63.3%) patients. Twenty-seven (90%) successfully underwent staged repair at 6.1 (4.5-8.2) months age. Follow-up was complete at a median duration of 46.9 (21.7-159.9) months. All patients survived the operation and are in good health at follow-up. Median ventilation time, ICU and hospital stay were 1 (1-2), 3 (2-5) and 23.5 (14-40) days, respectively. No patient developed any neurological complication. Three developed left subclavian artery thrombosis, one requiring surgical revision. With one unrelated late accidental death 14 years after neonatal repair, Kaplan-Meier survival was 90.9 [50.8-98.7]% at 15 years. Two patients underwent arch re-enlargement at the inner curvature to accommodate the DKS during stage 2, resulting in freedom from reoperation of 93.3[75.9-98.3]% at 10 years. All survivors enjoy subjective normal exercise tolerance with no relevant gradient. No patient is on anti-hypertensive medication. Median Z value of the proximal, transverse and distal arch was normalized to -0.88 (-2.19 to -0.12), -0.66(-1.33 to 0.08) and 0.34 (-0.10 to 1.33), respectively, at the last follow-up. Twenty-three (76.7%) arches achieved Romanesque shape at follow-up.
Conclusions: Long-term results of this minimally invasive approach show proportional growth without relevant gradient, freedom from hypertension and a Roman arch form, thus making it the preferred approach.
Keywords: Roman arch; aortic arch hypoplasia; aortic arch repair; coarctation; hypertension.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures



References
LinkOut - more resources
Full Text Sources
