

Impact of the establishment of a multidisciplinary national chronic thromboembolic pulmonary hypertension board on a monocentric surgical endarterectomy program
- PMID: 40036564
- PMCID: PMC11897790
- DOI: 10.1093/icvts/ivaf040
Impact of the establishment of a multidisciplinary national chronic thromboembolic pulmonary hypertension board on a monocentric surgical endarterectomy program
Abstract
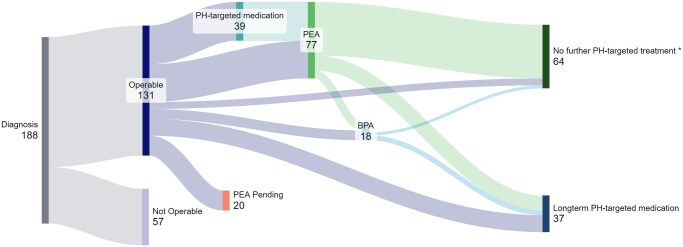
Objectives: Chronic thromboembolic pulmonary hypertension is a rare disease, characterized by delays in diagnosis and curative surgical treatment. After establishing a surgical pulmonary endarterectomy centre in Switzerland and due to a historically low resection rate of 14%, a national multidisciplinary evaluation board was established in January 2018. Herein, we summarize the impact of the board on our programme.
Methods: Patients discussed in the national chronic thromboembolic pulmonary hypertension board from January 2018 to December 2023 were included. Clinical characteristics, treatment allocation and survival were compared between patients undergoing surgery, patients refusing surgery and non-operable patients. Fisher's exact test or three-way ANOVA and Kaplan-Meier analyses were used.
Results: 188 patients were discussed at our national chronic thromboembolic pulmonary hypertension board; 131 (70%) presented with operable disease, 77 (41%) were referred for pulmonary endarterectomy and 34 (18%) of operable patients declined surgery. There is a significant difference in survival between these groups (P = 0.048). One- and 2-year survival in the subgroup undergoing pulmonary endarterectomy was 97% and 79%, respectively, while 1- and 2-year survival in the subgroup refusing pulmonary endarterectomy was 91% and 76%, respectively. The pulmonary endarterectomy rate has increased from a historical low of 14-41% since establishing the board.
Conclusions: Establishing an interdisciplinary board is essential to address diagnostic and management challenges in chronic thromboembolic pulmonary hypertension patients. The Swiss national chronic thromboembolic pulmonary hypertension board played an important role in substantially increasing the rate of curative surgery.
Keywords: chronic thromboembolic pulmonary hypertension; multidisciplinary board; pulmonary endarterectomy.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures






References
-
- Opitz I, Ulrich S. Chronic thromboembolic pulmonary hypertension. Swiss Med Wkly 2018;148:w14702. - PubMed
-
- Humbert M, Kovacs G, Hoeper MM et al.; ESC/ERS Scientific Document Group. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2022;43:3618–731. - PubMed
-
- Klok FA, Barco S, Konstantinides SV et al. Determinants of diagnostic delay in chronic thromboembolic pulmonary hypertension: results from the European CTEPH Registry. Eur Respir J 2018;52:P2612. - PubMed
-
- Delcroix M, Vonk Noordegraaf A, Fadel E, Lang I, Simonneau G, Naeije R. Vascular and right ventricular remodelling in chronic thromboembolic pulmonary hypertension. Eur Respir J 2013;41:224–32. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
