

Interplay between iron metabolism, inflammation, and EPO-ERFE-hepcidin axis in RDEB-associated chronic anemia
- PMID: 40036737
- PMCID: PMC12127647
- DOI: 10.1182/bloodadvances.2024015271
Interplay between iron metabolism, inflammation, and EPO-ERFE-hepcidin axis in RDEB-associated chronic anemia
Abstract
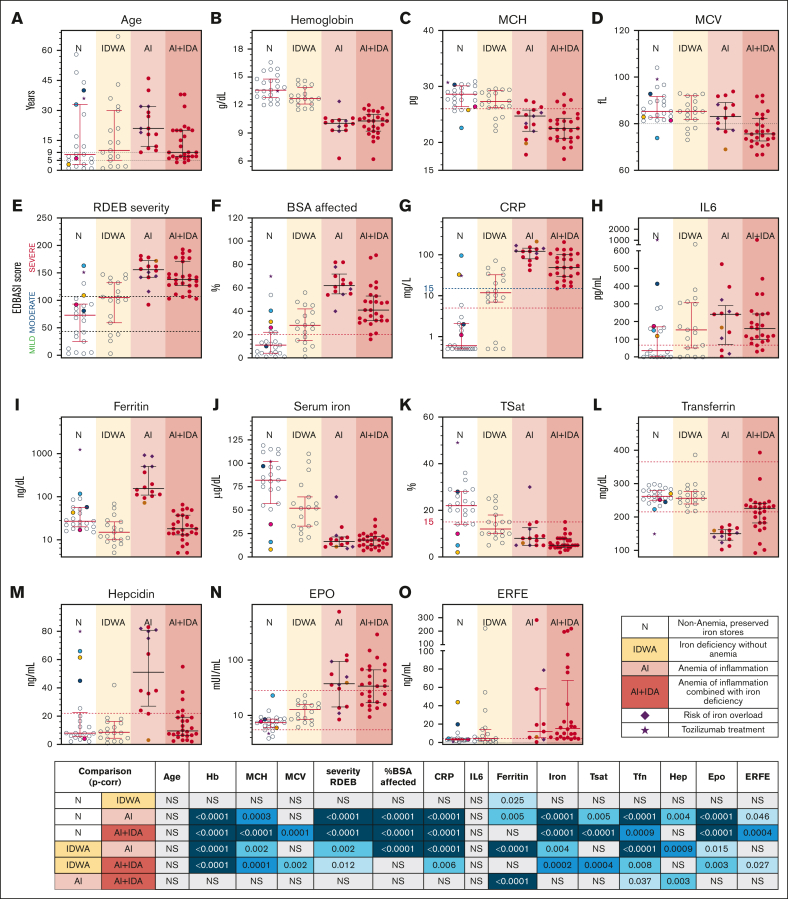
Recessive dystrophic epidermolysis bullosa (RDEB) is a genodermatosis characterized by severe cutaneous and mucosal fragility, and frequently complicated by multifactorial chronic anemia that responds poorly to conventional therapies. This cross-sectional study investigates the factors contributing to anemia in RDEB by analyzing a representative cohort, that was stratified by disease severity, anemia, and iron status, to examine their hematological parameters, cytokine profile, and the erythropoietin-erythroferrone-hepcidin (EPO-ERFE-hepcidin) axis. Anemia was present in 50% of the cohort. Hemoglobin levels showed a strong negative correlation with the percentage of body surface area affected and C-reactive protein levels (CRP), identifying these as anemia risk factors in RDEB. Moderate-severe inflammation (CRP ≥ 15 mg/L) was observed in all patients with anemia, but no specific cytokine profile was linked with anemia risk because of variability in interleukin-6 (IL-6), IL-1β, IL-10, tumor necrosis factor, and interferon-γ levels. The regulation of the EPO-ERFE-hepcidin axis showed discrepancies with the patterns expected based on patients' anemia severity and iron status. According to the reticulocyte production index, an inadequate bone marrow response was observed in 90% of patients with anemia, irrespective of EPO levels. Patients with functional or true iron deficiency had higher ERFE levels, although ERFE showed no consistent correlation with EPO and was elevated in both patients with anemia and those without anemia. Elevated hepcidin was primarily linked to the highest ferritin levels, mostly in patients with a history of iron infusions and/or transfusions. These findings highlight the need for personalized, targeted approaches that address the complex interplay between inflammation and iron dysregulation, to improve anemia management in RDEB and other chronic inflammatory conditions.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures







References
-
- Bardhan A, Bruckner-Tuderman L, Chapple ILC, et al. Epidermolysis bullosa. Nat Rev Dis Primers. 2020;6(1):78. 27. - PubMed
-
- Tarango C, Quinn CT, Augsburger B, Lucky AW. Iron status and burden of anemia in children with recessive dystrophic epidermolysis bullosa. Pediatr Dermatol. 2023;40(2):288–293. - PubMed
-
- Reimer A, Hess M, Schwieger-Briel A, et al. Natural history of growth and anaemia in children with epidermolysis bullosa: a retrospective cohort study. Br J Dermatol. 2020;182(6):1437–1448. - PubMed
-
- Popp C, Miller W, Eide C, Tolar J, McGrath JA, Ebens CL. Beyond the surface: a narrative review examining the systemic impacts of recessive dystrophic epidermolysis bullosa. J Invest Dermatol. 2024;144(9):1943–1953. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
