

High intensity exercise programme in patients with hypertrophic cardiomyopathy: a randomized trial
- PMID: 40037382
- PMCID: PMC12075935
- DOI: 10.1093/eurheartj/ehae919
High intensity exercise programme in patients with hypertrophic cardiomyopathy: a randomized trial
Abstract
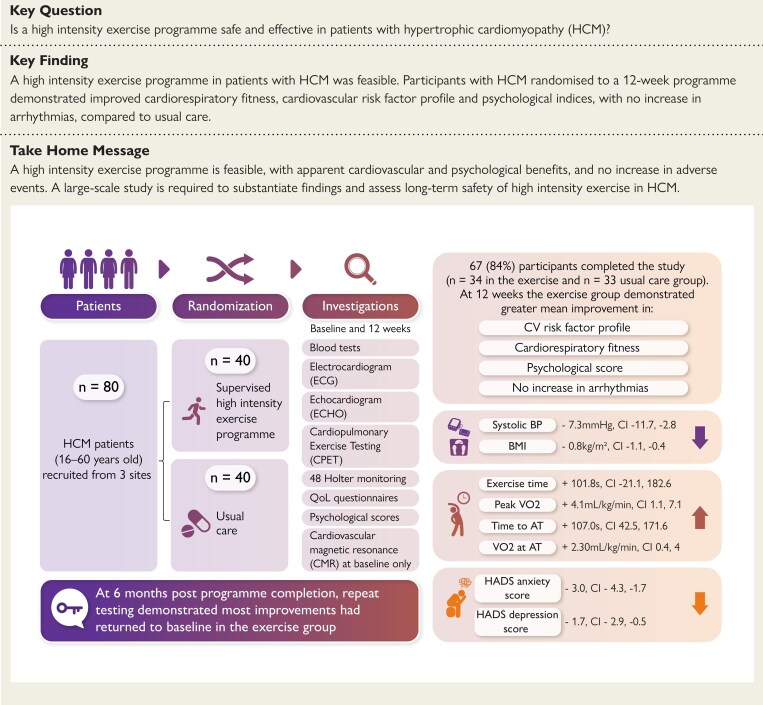
Background and aims: The feasibility and impact of high intensity exercise programmes in patients with hypertrophic cardiomyopathy (HCM) are unknown. This study was conducted to determine the feasibility of a high intensity exercise programme and explore safety and efficacy outcomes in patients with HCM.
Methods: Participants were randomized to a 12-week supervised exercise programme (n = 40) in addition to usual care, or usual care alone (n = 40). All participants underwent assessment at baseline and 12 weeks. The exercise group was re-evaluated 6 months post-programme. Feasibility was assessed by (i) recruitment, adherence, and retention rates; (ii) staffing ratios; (iii) logistics; and (iv) acceptability of the intervention. The primary exploratory safety outcome was a composite of arrhythmia-related events. Exploratory secondary outcomes included changes in (i) cardiorespiratory fitness; (ii) cardiovascular risk factors; and (iii) quality of life, anxiety, and depression scores.
Results: Overall, 67 (84%) participants completed the study (n = 34 and n = 33 in the exercise and usual care groups, respectively). Reasons for non-adherence included travel, work, and family commitments. Resource provision complied with national cardiac rehabilitation standards. There was no difference between groups for the exploratory safety outcome (P = .99). At 12 weeks, the exercise group had a greater increase in peak oxygen consumption (VO2) [+4.1 mL/kg/min, 95% confidence interval (CI) 1.1, 7.1] and VO2 at anaerobic threshold (+2.3 mL/kg/min, 95% CI 0.4, 4.1), lower systolic blood pressure (-7.3 mmHg, 95% CI -11.7, -2.8) and body mass index (-0.8 kg/m2, 95% CI -1.1, -0.4), and greater improvement in hospital anxiety (-3, 95% CI -4.3, -1.7) and depression (-1.7, 95% CI -2.9, -0.5) scores, compared to the usual care group. Most exercise gains dissipated at 6 months.
Conclusions: A high intensity exercise programme is feasible in patients with HCM, with apparent cardiovascular and psychological benefits, and no increase in arrhythmias. A large-scale study is required to substantiate findings and assess long-term safety of high intensity exercise in HCM.
Keywords: Cardiac rehabilitation; High intensity exercise; Hypertrophic cardiomyopathy; Sports cardiology.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures



References
-
- Pelliccia A, Fagard R, Bjørnstad HH, Anastassakis A, Arbustini E, Assanelli D, et al. Recommendations for competitive sports participation in athletes with cardiovascular disease: a consensus document from the Study Group of Sports Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J 2005;26:1422–45. 10.1093/eurheartj/ehi325 - DOI - PubMed
-
- Maron BJ, Udelson JE, Bonow RO, Nishimura RA, Ackerman MJ, Estes NAM, et al. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 3: hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and other cardiomyopathies, and myocarditis: a scientific statement from the American Heart Association and American College of Cardiology. Circulation 2015;132:e273–280. 10.1161/CIR.0000000000000239 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
