

Effect of statin therapy on coronary inflammation assessed by pericoronary adipose tissue computed tomography attenuation
- PMID: 40037525
- PMCID: PMC12042745
- DOI: 10.1093/ehjci/jeaf062
Effect of statin therapy on coronary inflammation assessed by pericoronary adipose tissue computed tomography attenuation
Abstract
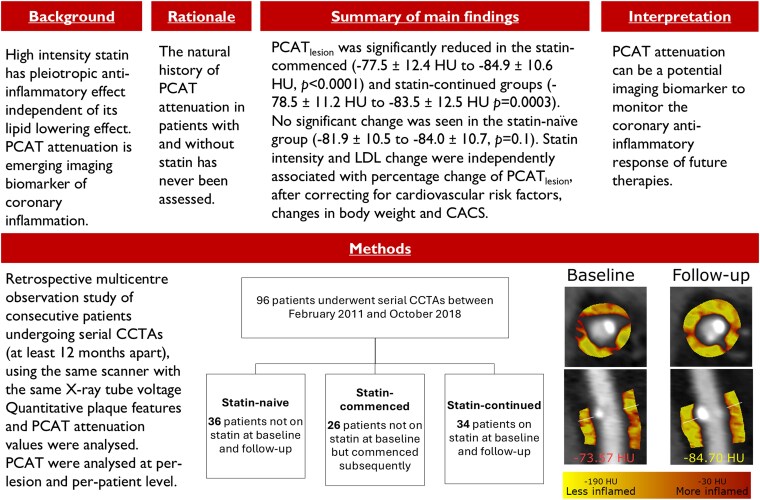
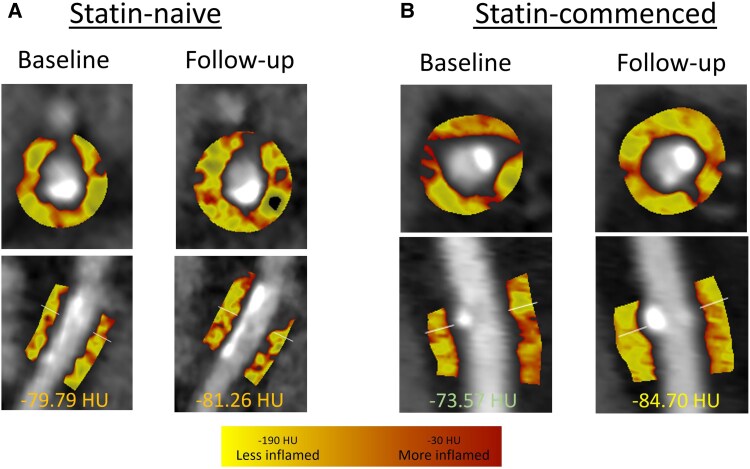
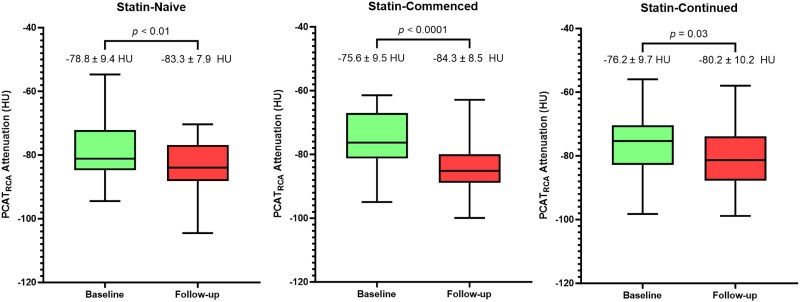
Aims: Pericoronary adipose tissue (PCAT) attenuation on coronary computed tomography angiography (CCTA) is an imaging biomarker of coronary inflammation. The natural history of PCAT attenuation remains unknown. High-intensity statin therapy has pleiotropic anti-inflammatory effects. We sought to assess temporal changes in PCAT attenuation in patients with and without statin therapy.
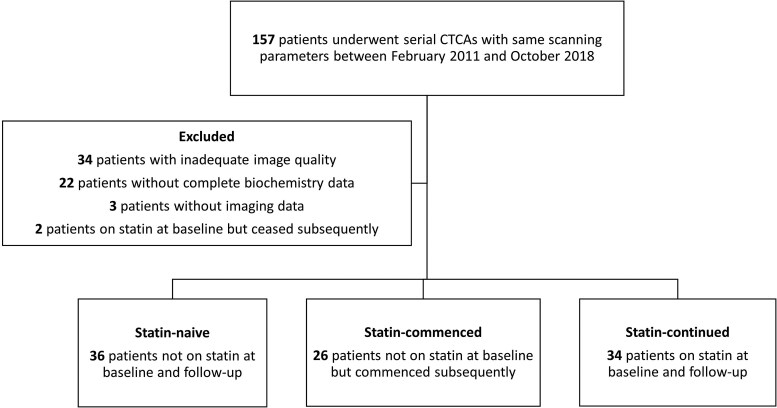
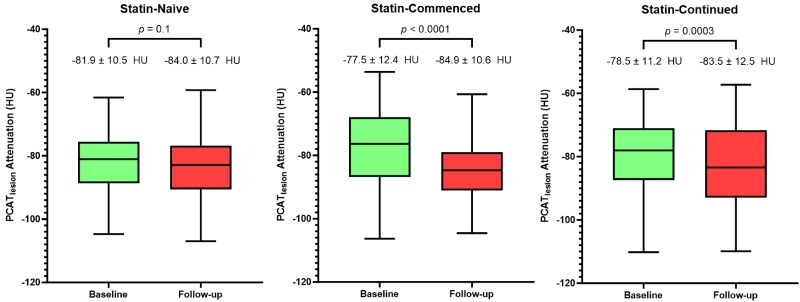
Methods and results: This was a multicentre observational study that included consecutive patients with stable coronary artery disease (CAD) undergoing clinically indicated serial CCTA with identical scan parameters ≥ 12 months apart between May 2013 and July 2022. Using semi-automated software, PCAT attenuation was measured on a per-lesion level (PCATlesion) and per-patient level around the proximal right coronary artery (PCATRCA). Of the 96 patients (57 ± 11 years, 60% male), 34 patients were not on a statin at baseline or follow-up (statin-naive), 26 patients were commenced on a statin after the baseline scan (statin-commenced), and 34 patients were on a statin at both time points (statin-continued). There was no significant difference between the groups for age, sex, body mass index (BMI), and prevalence of traditional cardiovascular risk factors except for dyslipidaemia (25.0% vs. 34.6% vs. 64.7%, P < 0.01 for trend). At a median follow-up of 3.8 years, there was a significant reduction in PCATlesion in the statin-commenced (-79.4 ± 11.7 to -86.5 ± 10 HU, P < 0.001) and the statin-continued (-83.5 ± 8.5 to -90.6 ± 8.5 HU, P = 0.001) groups. Meanwhile, no significant difference in PCATlesion was observed in the statin-naïve group (-84.4 ± 9.7 to -86.6 ± 9.5, P = 0.1). Multivariate analysis showed statin intensity and LDL change to be independently associated with percentage change of PCATlesion, after correcting for cardiovascular risk factors, changes in body weight, and coronary artery calcium score.
Conclusion: Statin therapy was associated with a reduction in PCATlesion, while no significant change in PCATlesion was observed without statin therapy. If validated in larger studies, PCAT attenuation could potentially be used to monitor the response of the coronary arteries to statins and guide treatment.
Keywords: atherosclerosis; coronary computed tomography angiography; inflammation; pericoronary adipose tissue; statin.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
Similar articles
-
Pericoronary Adipose Tissue CT Attenuation in Kawasaki Disease and Association with Coronary Artery Aneurysms, Myocardial Perfusion, and Coronary Events.Radiol Cardiothorac Imaging. 2025 Jun;7(3):e240303. doi: 10.1148/ryct.240303. Radiol Cardiothorac Imaging. 2025. PMID: 40569153 Clinical Trial.
-
Pericoronary Adipose Tissue Attenuation in Patients with Future Acute Coronary Syndromes: The ICONIC Study.Radiol Cardiothorac Imaging. 2025 Jun;7(3):e240200. doi: 10.1148/ryct.240200. Radiol Cardiothorac Imaging. 2025. PMID: 40539913
-
Right coronary artery pericoronary fat attenuation index as a future predictor for acute coronary events in nonobstructive coronary artery disease - a prospective single centre study.Clin Radiol. 2025 Mar;82:106774. doi: 10.1016/j.crad.2024.106774. Epub 2024 Dec 12. Clin Radiol. 2025. PMID: 39847939
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.Health Technol Assess. 2006 Oct;10(39):iii-iv, ix-x, 1-41. doi: 10.3310/hta10390. Health Technol Assess. 2006. PMID: 17018228
-
Association of Pericoronary Adipose Attenuation With Major Adverse Cardiovascular Events and High-Risk Plaque.JACC Cardiovasc Imaging. 2025 Aug;18(8):884-894. doi: 10.1016/j.jcmg.2025.04.008. Epub 2025 Jul 10. JACC Cardiovasc Imaging. 2025. PMID: 40643422
Cited by
-
Computed tomography-based assessment of pericoronary adipose tissue in cardiovascular diseases: Diagnostic and prognostic implications.World J Radiol. 2025 Jun 28;17(6):107281. doi: 10.4329/wjr.v17.i6.107281. World J Radiol. 2025. PMID: 40606053 Free PMC article. Review.
References
-
- Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation 2002;105:1135–43. - PubMed
-
- Camici PG, Rimoldi OE, Gaemperli O, Libby P. Non-invasive anatomic and functional imaging of vascular inflammation and unstable plaque. Eur Heart J 2012;33:1309–17. - PubMed
-
- Antonopoulos AS, Sanna F, Sabharwal N, Thomas S, Oikonomou EK, Herdman Let al. . Detecting human coronary inflammation by imaging perivascular fat. Sci Transl Med 2017;9:eaal2658. - PubMed
-
- Oikonomou EK, Marwan M, Desai MY, Mancio J, Alashi A, Centeno EHet al. . Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data. The Lancet 2018;392:929–39. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
