

Emerging role of IGF1R and IR expression and localisation in adrenocortical carcinomas
- PMID: 40038716
- PMCID: PMC11877998
- DOI: 10.1186/s12964-025-02115-0
Emerging role of IGF1R and IR expression and localisation in adrenocortical carcinomas
Abstract
Background: The insulin-like growth factor 2 (IGF2) is overexpressed in 90% of adrenocortical carcinomas (ACC) and promotes cell proliferation via IGF1R and isoform A of insulin receptor (IRA). However, IGF2 role in ACC tumourigenesis has not been completely understood yet, and the contribution of IGF1R and IRA in mediating ACC cell growth has been poorly explored. This study aimed to investigate IGF1R and IR expression and localisation, including the expression of IR isoforms, in ACC and adrenocortical adenomas (ACA), and their role in IGF2-driven proliferation.
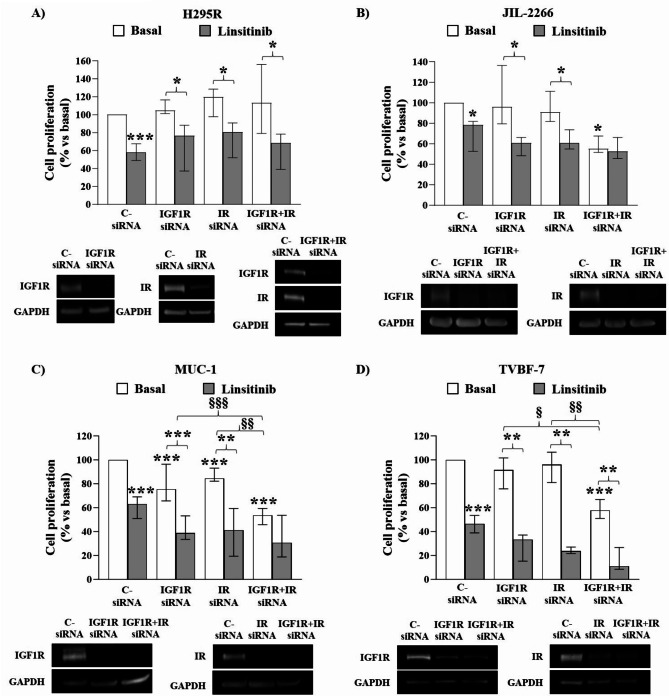
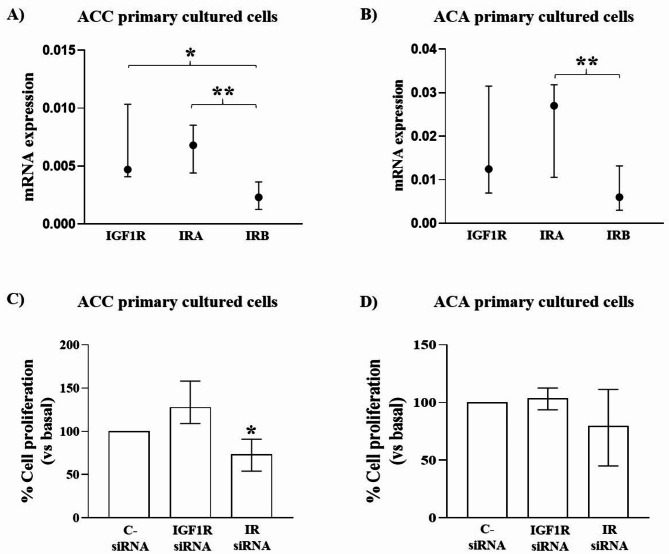
Methods: Immunohistochemistry staining of IGF1R and IR was performed on 118 ACC and 22 ACA to evaluate their expression and cellular localisation and statistical analyses were carried out to assess correlations with clinicopathological data. The expression of IRA and IRB in ACC and ACA tissues, ACC cell lines and ACC and ACA primary cultures was determined by RT-qPCR. To appraise the specific role of IGF1R and IR in mediating IGF2 mitogenic pathway, single and double silencing of receptors and their inhibition in 2 ACC cell lines derived from primary tumours (H295R and JIL-2266) and 2 derived from metastatic tumours (MUC-1 and TVBF-7) as well as in ACC and ACA primary cultures were performed.
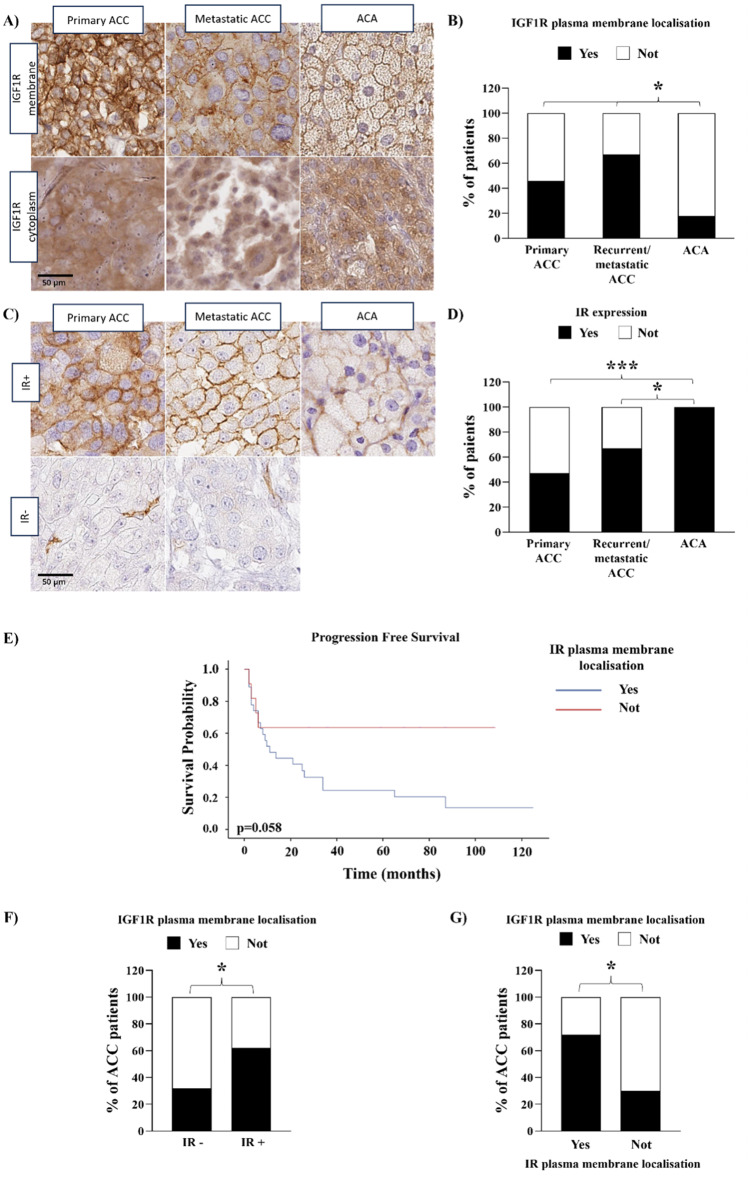
Results: We found a higher IGF1R plasma membrane localisation in ACC compared to ACA. In ACC this localisation was associated with higher Ki67 and Weiss score. IR was expressed in about half of ACC and in all ACA but, in ACC, it was associated with higher Ki67 and Weiss score. RT-qPCR revealed that the prevalent isoform of IR was IRA in ACC and ACA, but not in normal adrenals. In ACC cell lines, double IGF1R + IR silencing reduced cell proliferation in JIL-2266, MUC-1 and TVBF-7 but not in H295R. In ACC, but not ACA, primary cultures, cell proliferation was reduced after IR but not IGF1R knockdown.
Conclusions: Overall, these data suggest that IGF1R localisation and IR expression represent new biomarkers predicting tumour aggressiveness, as well as possible molecular markers useful to patients' stratification for more individualized IGF1R-IR targeted therapies or for novel pharmacological approaches specifically targeting IRA isoform.
Keywords: Adrenocortical carcinoma; Biomarker; Cellular localisation; IGF1R; Insulin receptor.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki and approved by Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico Ethics Committee (Comitato Etico Milano Area 2, protocol code 20_2019bis, date of approval 18 January 2019 and protocol code 554_2022bis, date of approval 9 June 2022), by the local ethics committee of the University of Wuerzburg (#88/11 for the ENSAT Registry), by Careggi University Hospital Ethical Committee (Protocol code 2011/0020149—Rif CEAVC Em.2019 − 201, date of approval 26 November 2019), by the Ethical Committee of the Institutional Board of Laikon General Hospital (Protocol code 4/17.01.2022, date of approval 17 January 2022) and by the Ethical Committee of the Area Vasta Emilia Centro (CE-AVEC, Protocol code: 105/2017/U/Tess). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Fassnacht M, Johanssen S, Quinkler M, Bucsky P, Willenberg HS, Beuschlein F et al. German Adrenocortical Carcinoma Registry Group; European Network for the Study of Adrenal Tumors. Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: proposal for a Revised TNM Classification. Cancer 2009;115:243– 50. 10.1002/cncr.24030. PMID: 19025987. - PubMed
-
- Lippert J, Fassnacht M, Ronchi CL. The role of molecular profiling in adrenocortical carcinoma. Clin Endocrinol (Oxf) 2022;97:460– 72. 10.1111/cen.14629. PMID: 34750847. - PubMed
-
- Amodru V, Garcia ME, Libe R, Brue T, Reznik Y, Castinetti F. Medical management of adrenocortical carcinoma: Current recommendations, new therapeutic options and future perspectives. Ann Endocrinol (Paris). 2021;82:52– 8. 10.1016/j.ando.2020.12.003. PMID: 33279475. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
