

A real-world study on the influence of unplanned reoperations on hospitalized patients using the diagnosis-related group
- PMID: 40038862
- PMCID: PMC11884101
- DOI: 10.1080/07853890.2025.2473633
A real-world study on the influence of unplanned reoperations on hospitalized patients using the diagnosis-related group
Abstract
Objective: The issue of unplanned reoperations poses significant challenges within healthcare systems, with assessing their impact being particularly difficult. The current study aimed to assess the influence of unplanned reoperations on hospitalized patients by employing the diagnosis-related group (DRG) to comprehensively consider the intensity and complexity of different medical services.
Methods: A retrospective cohort study of surgical patients was conducted at a large tertiary hospital with two hospital districts employing data sourced from a DRG database. Hospital length of stay (LOS) and hospitalization costs were measured as the primary outcomes. Discharge to home was measured as the secondary outcome. Frequency matching based on DRG, regression modeling, subgroup comparison and sensitivity analysis were applied to evaluate the influence of unplanned reoperations.
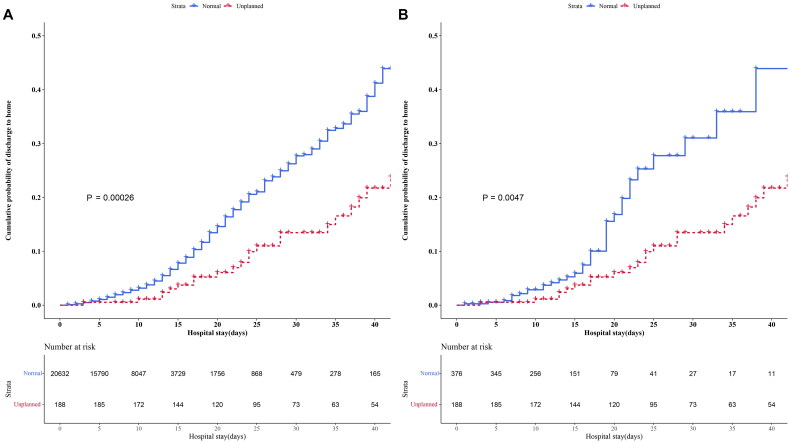
Results: We identified 20820 surgical patients distributed across 79 DRGs, including 188 individuals who underwent unplanned reoperations and 20632 normal surgical patients in the same DRGs. After DRG-based frequency matching, 564 patients (188 with unplanned reoperations, 376 normal surgical patients) were included. Unplanned reoperations led to prolonged LOS (before matching: adjusted difference, 12.05 days, 95% confidence interval [CI] 10.36-13.90 days; after matching: adjusted difference, 14.22 days, 95% CI 11.36-17.39 days), and excess hospitalization costs (before matching: adjusted difference, $4354.29, 95% CI: $3,817.70-$4928.67; after matching: adjusted difference, $5810.07, 95% CI $4481.10-$7333.09). Furthermore, patients who underwent unplanned reoperations had a reduced likelihood of being discharged to home (before matching: hazard ratio [HR] 0.27, 95% CI 0.23-0.32; after matching: HR 0.31, 95% CI 0.25-0.39). Subgroup analyses indicated that the outcomes across the various subgroups were mostly uniform. In high-level surgery subgroups (levels 3-4) and in relation to complex diseases (relative weight ≥ 2), the increase in hospitalization costs and LOS was more pronounce after unplanned reoperations. Similar results were observed with sensitivity analysis by propensity score matching and excluding short LOS.
Conclusions: Incorporating the DRG allows for a more effective assessment of the influence of unplanned reoperations. In managing such reoperations, mitigating their influence, especially in the context of high-level surgeries and complex diseases, remains a significant challenge that requires special consideration.
Keywords: Unplanned reoperation; diagnosis-related group; discharge to home; hospital length of stay; hospitalization cost; retrospective cohort study.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures



Similar articles
-
The influence of adverse events on inpatient outcomes in a tertiary hospital using a diagnosis-related group database.Sci Rep. 2024 Aug 5;14(1):18114. doi: 10.1038/s41598-024-69283-w. Sci Rep. 2024. PMID: 39103554 Free PMC article.
-
Impact of healthcare-associated infection on healthcare services and survival of patients with cancer: a propensity score-matched retrospective study.BMC Cancer. 2025 Apr 1;25(1):595. doi: 10.1186/s12885-025-13975-7. BMC Cancer. 2025. PMID: 40170132 Free PMC article.
-
The Frank Stinchfield Award : Total Hip Arthroplasty for Femoral Neck Fracture Is Not a Typical DRG 470: A Propensity-matched Cohort Study.Clin Orthop Relat Res. 2017 Feb;475(2):353-360. doi: 10.1007/s11999-016-4868-2. Clin Orthop Relat Res. 2017. PMID: 27154530 Free PMC article.
-
Conversion THA With Concomitant Removal of Orthopaedic Hardware Should Be Reclassified as a Revision Surgery in the Medicare Severity Diagnosis-Related Group Coding Scheme: An Analysis of Cost and Resource Use.Clin Orthop Relat Res. 2024 May 1;482(5):790-800. doi: 10.1097/CORR.0000000000002894. Epub 2023 Oct 18. Clin Orthop Relat Res. 2024. PMID: 37851410 Free PMC article.
-
The impact of diagnosis-related group-based medical insurance payment model on the prognosis and nursing care of patients undergoing composite trabeculectomy: a retrospective cohort study.Front Public Health. 2025 May 21;13:1518546. doi: 10.3389/fpubh.2025.1518546. eCollection 2025. Front Public Health. 2025. PMID: 40469599 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources