

Multiomics insights into BMI-related intratumoral microbiota in gastric cancer
- PMID: 40041144
- PMCID: PMC11876552
- DOI: 10.3389/fcimb.2025.1511900
Multiomics insights into BMI-related intratumoral microbiota in gastric cancer
Abstract
Introduction: Body mass index (BMI) is considered an important factor in tumor prognosis, but its role in gastric cancer (GC) remains controversial. There is a lack of studies exploring the effect of BMI on gastric cancer from the perspective of intratumoral microbiota. This study aimed to compare and analyze the differences in and functions of intratumoral microbiota among GC patients with varying BMIs, aiming to ascertain whether specific microbial features are associated with prognosis in low-BMI (LBMI) gastric cancer patients.
Methods: A retrospective analysis of the clinicopathological features and prognosis of 5567 patients with different BMIs was performed between January 2010 and December 2019. Tumor tissues from 189 GC patients were collected for 16S rRNA sequencing, 64 samples were selected for transcriptome sequencing, and 57 samples were selected for untargeted metabolomic analysis.
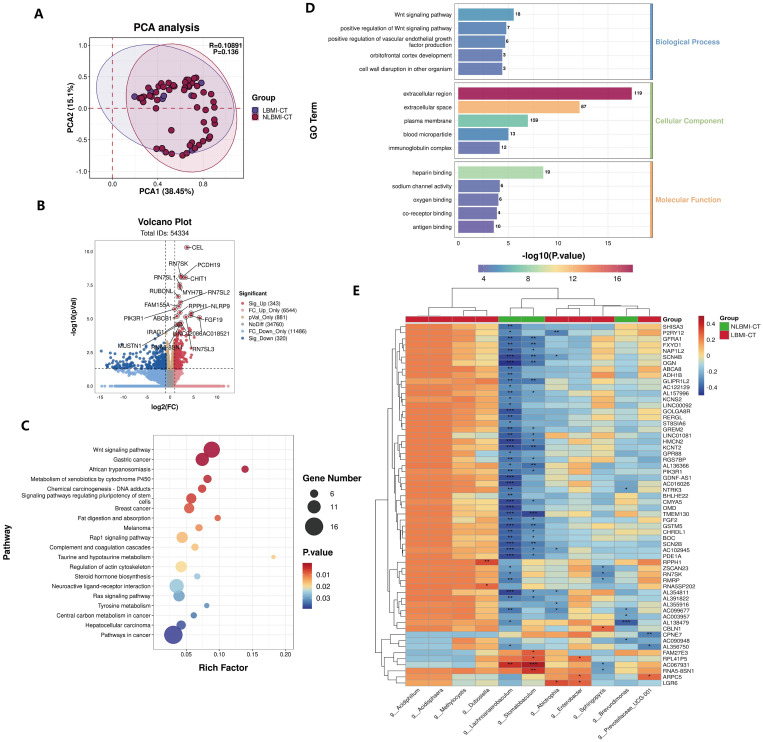
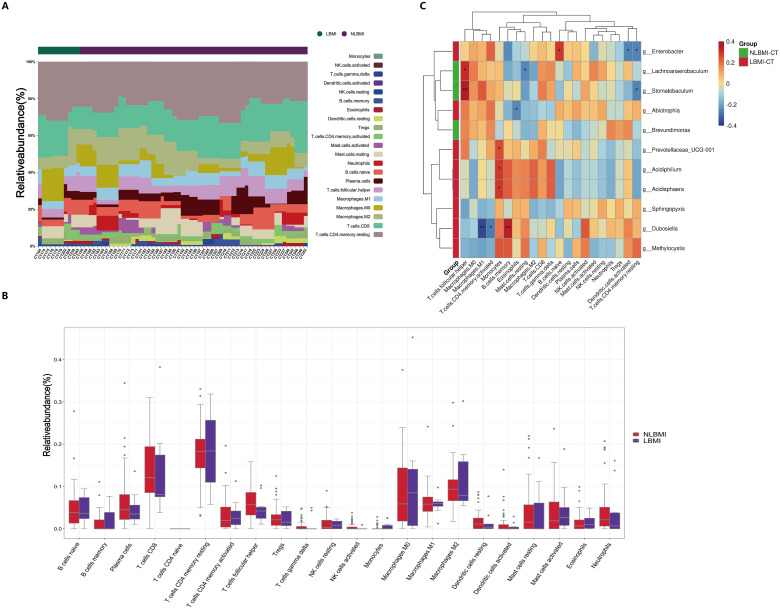
Results: Clinical cohort analysis revealed that GC patients with a low BMI presented poorer clinical and pathological characteristics than those with a non-low-BMI (NLBMI). LBMI was identified as a significant independent risk factor for adverse prognosis, potentially exerting immunosuppressive effects on postoperative adjuvant chemotherapy. 16S rRNA sequencing revealed no significant differences in the alpha and beta diversity of the intratumoral microbiota between the two groups of GC patients. However, LEfSe analysis revealed 32 differential intratumoral microbiota between the LBMI and NLBMI groups. Notably, the genus Abiotrophia was significantly enriched in the LBMI group. Further in-depth analysis indicated that the genus Abiotrophia was inversely associated with eosinophils, P2RY12, and SCN4B genes, and positively linked with LGR6 in LBMI gastric cancer patients. Metabolomic assessments revealed that LBMI was positively associated with purine metabolites, specifically guanine and inosine diphosphate (IDP).
Discussion: In conclusion, LBMI is an independent risk factor for poor prognosis in gastric cancer patients and may have an inhibitory effect on postoperative adjuvant chemotherapy. Intratumor flora of gastric cancer patients with different BMI levels differed, with different immune cell infiltration and metabolic characteristics. The genus Abiotrophia may promote gastric cancer development and progression by regulating eosinophils and the purine metabolism pathway, which provides a new idea for the precise treatment of gastric cancer.
Keywords: BMI; GC; immune cells; intratumoral microbiota; metabolome.
Copyright © 2025 Liu, Jiang, Ma, Xia, Zheng, Yin, Pang, Yuan, Cheng, Liu, Zhang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Amin M. B., Greene F. L., Edge S. B., Compton C. C., Gershenwald J. E., Brookland R. K., et al. . (2017). The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA: A Cancer J. Clin. 67, 93–99. doi: 10.3322/caac.21388 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous