

The effect of an exam-indicated cerclage before 24 weeks of gestation to prevent preterm birth: A systematic review and meta-analysis
- PMID: 40041371
- PMCID: PMC11876763
- DOI: 10.1016/j.eurox.2025.100372
The effect of an exam-indicated cerclage before 24 weeks of gestation to prevent preterm birth: A systematic review and meta-analysis
Abstract
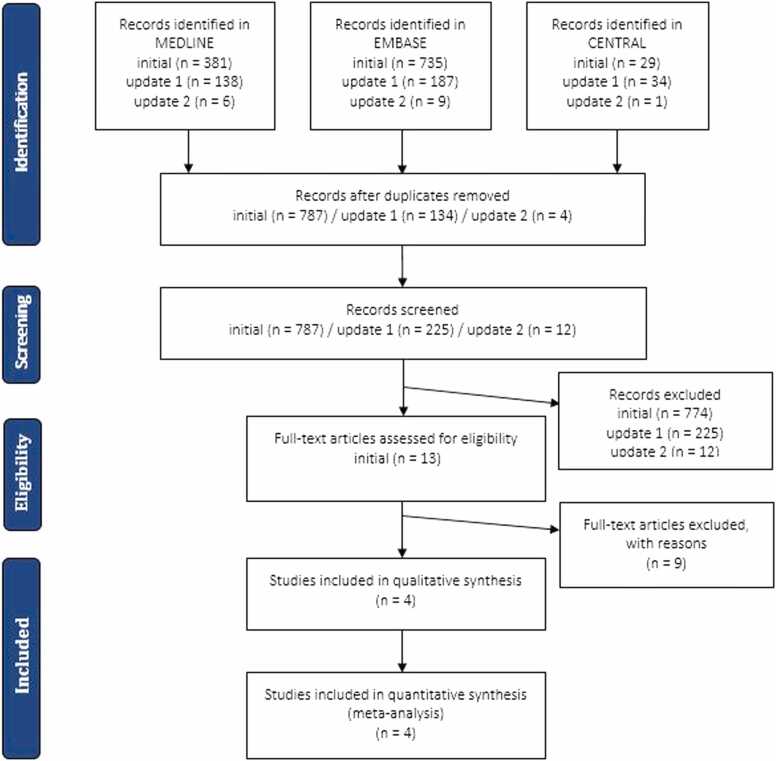
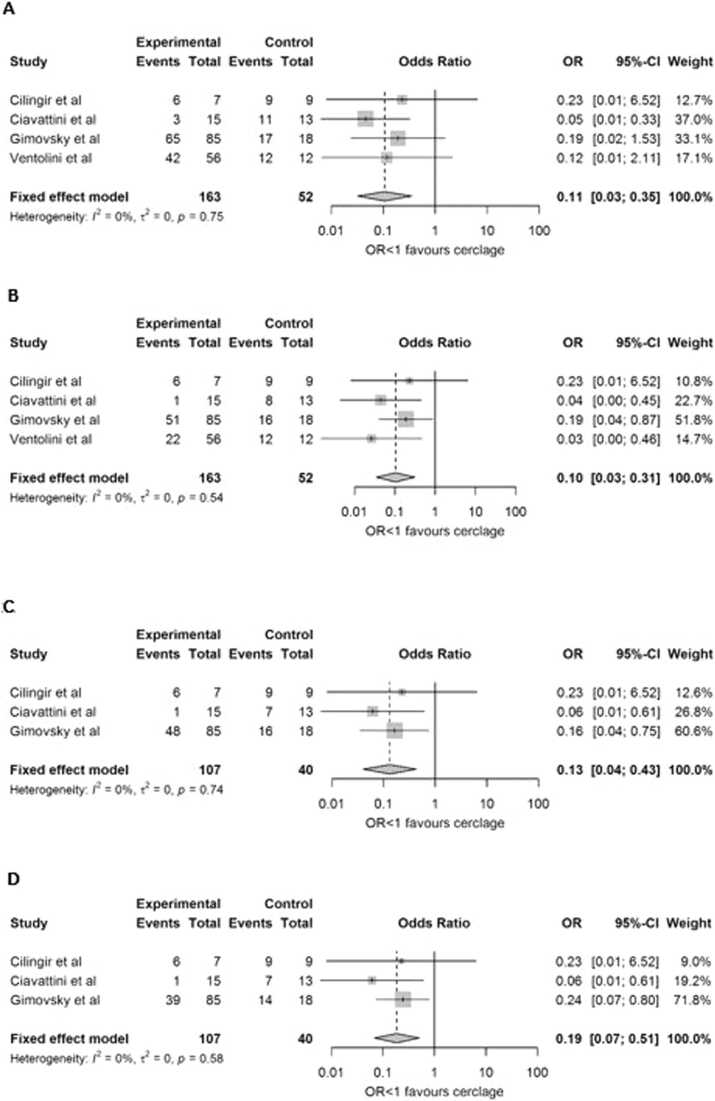
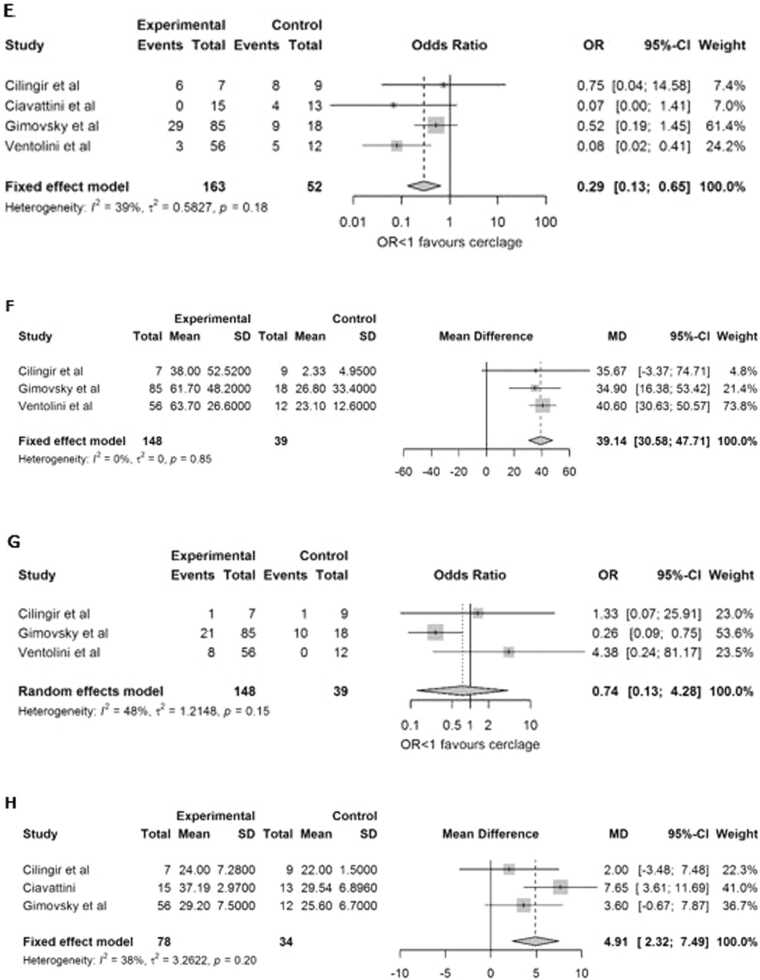
The effect of an exam-indicated cerclage (EIC) remains uncertain due to limited evidence from reviews covering pregnancies beyond this timeframe. With the 24-week mark serving as an international threshold for neonatal care initiation, the aim of this systematic review was to evaluate the available literature on the effectiveness of an EIC before 24 weeks of gestation. MEDLINE, EMBASE, Web of Science, CENTRAL, clinicaltrials.gov and WHO-ICTRP were searched for randomized controlled trials, cohort and case-control studies comparing EIC with expectant management in singleton pregnancies with cervical dilation ≤ 5 cm between 14 and 24 weeks of gestation to prevent preterm birth (PTB) < 37 weeks of gestation. Secondary outcomes included obstetrical and neonatal outcomes. Quality assessment was preformed using Newcastle-Ottawa Scale. Analyses were conducted using R(studio) version 3.6.1. and outcomes stated as odds ratios (OR) with 95 % confidence intervals (CI). Prospero: #CRD42019137400. The search yielded 787 potential studies. Four studies non-randomized (retrospective) could be included. Quality assessment showed overall good quality. The main weaknesses were retrospective designs, small sample sizes and the poor comparability of the intervention and control groups. The study population resulted in 215 women, among whom 163 (76 %) underwent cerclage placement and 52 (24 %) were expectantly managed. EIC compared with expectant management was associated with significant lower rates of PTB before 37 weeks (71.2 % vs 94.2 %; OR 0.11; 95 % CI 0.03-0.35), 34 weeks (49.1 % vs 86.5 %; OR 0.10; 95 % CI 0.03-0.31), 32 weeks (43.0 % vs 80.0 %; OR 0.13; 95 % CI 0.04-0.43), 28 weeks (43.0 % vs 75.0 %; OR 0.19; 95 % CI 0.07-0.51) and 24 weeks (23.3 % vs 50 %; OR 0.29; 95 % CI 0.13-0.65) of gestation, significant prolongation of the pregnancy (mean difference 39.14 days; 95 %CI 30.58-47.71; p-value <0.0001) and a greater gestational age at delivery (mean difference 4.91 weeks; 95 % CI 2.32-7.49; p-value 0.0002) compared to expectant management. The current literature suggests that EIC before 24 weeks of gestation is associated with improved pregnancy outcomes compared to expectant management. The results are limited by the lack of randomised trials and studied neonatal outcomes plus the potential for bias in the included studies.
Keywords: Cervical insufficiency; Emergency cerclage; Exam-indicated cerclage; Expectant management; Preterm birth; Spontaneous preterm birth; Viable age.
© 2025 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: B.W. Mol reports a relationship with National Health and Medical Research Council that includes: funding grants. B.W. MOL reports a relationship with Obs Eva that includes: consulting or advisory. B.W. MOL reports a relationship with Merck KGaA that includes: consulting or advisory and travel reimbursement. B.W. MOL reports a relationship with Guerbet that includes: consulting or advisory. B.W. MOL reports a relationship with Igenomix that includes: consulting or advisory. B.W. MOL reports a relationship with Merck & Co Inc that includes: consulting or advisory. M.O. Oudijk reports a relationship with Stichting stoptevroegbevallen that includes: board membership. E. Pajkrt reports a relationship with Stichting stoptevroegbevallen that includes: board membership. M.O. Oudijk reports a relationship with Fetal-Maternal Medicine NVOG that includes: board membership. M.O. Oudijk reports a relationship with Amsterdam Reproduction & Development Research Institute that includes: funding grants. M.O. Oudijk reports a relationship with Pregnolia that includes: funding grants. M.O. Oudijk reports a relationship with Netherlands Organisation for Health Research and Development that includes: funding grants. E. Pajkrt reports a relationship with Review Committee Late pregnancy termination and end of life decisions newborns appointed by the Ministry of Health and Ministry of Justice that includes: board membership. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Rand L., Norwitz E.R. Current controversies in cervical cerclage. Semin Perinatol. 2003;27(1):73–85. - PubMed
-
- Koullali B., Oudijk M.A., Nijman T.A., Mol B.W., Pajkrt E. Risk assessment and management to prevent preterm birth. Semin Fetal Neonatal Med. 2016;21(2):80–88. - PubMed
-
- Boelig R.C., Berghella V. Current options for mechanical prevention of preterm birth. Semin Perinatol. 2017;41(8):452–460. - PubMed
-
- Brown R., Gagnon R., Delisle M.F. No. 373-cervical insufficiency and cervical cerclage. J Obstet Gynaecol Can. 2019;41(2):233–247. - PubMed
-
- Shennan A., Jones B. The cervix and prematurity: aetiology, prediction and prevention. Semin Fetal Neonatal Med. 2004;9(6):471–479. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
