

Spinal metastases at the thoracolumbar junction - Influencing factors for surgical decision-making according to a multicentric registry
- PMID: 40041395
- PMCID: PMC11876765
- DOI: 10.1016/j.bas.2025.104198
Spinal metastases at the thoracolumbar junction - Influencing factors for surgical decision-making according to a multicentric registry
Abstract
Introduction: Spinal metastases at the thoracolumbar junction (TLJ) pose a significant risk for spinal instability and necessitate special considerations regarding surgical management. Longer patient survival due to improved oncologic therapies may justify extensive instrumented surgery.
Research question: The aim of this study was to analyze the standard of care in a large multicentric cohort of patients with TLJ metastases regarding surgical decision-making, management, and associated morbidity.
Material and methods: Patients with surgically treated spinal metastases at the TLJ between 2010 and 2022 were enrolled at five academic tertiary spine centers. Epidemiological, surgical, clinical, and outcome data was assessed retrospectively. Surgical management was sorted according to three groups: decompression ( i ), decompression and posterior instrumentation ( ii ), and decompression and 360° instrumentation with vertebral body replacement ( iii ). Sole biopsies or kypho-/vertebroplasties were excluded.
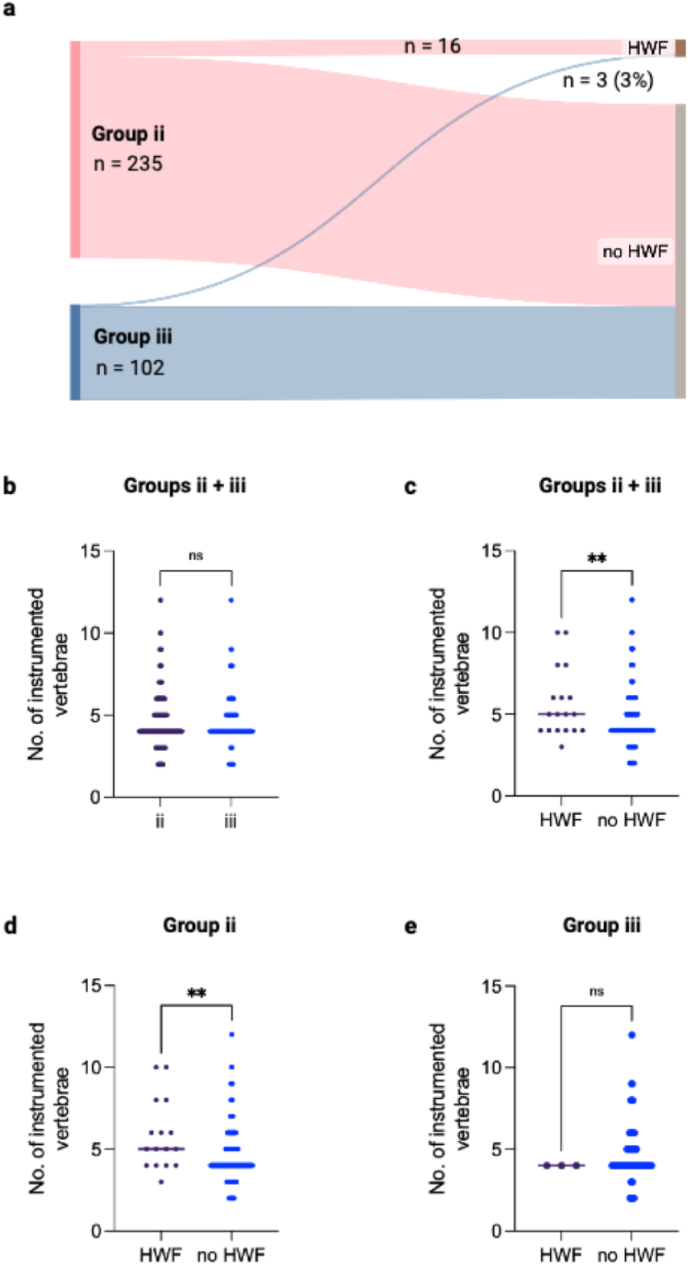
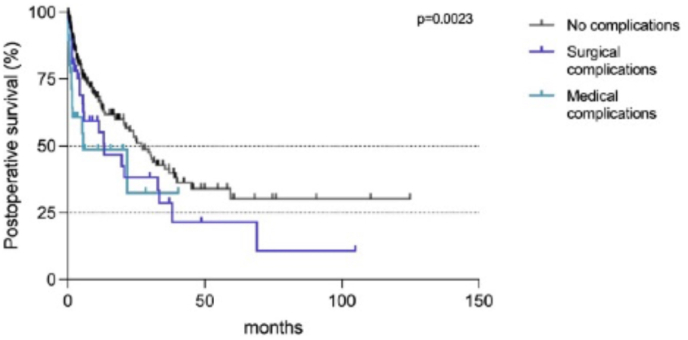
Results: The inclusion criteria was met by 396 patients, of which 59 (15%) were treated with decompression ( i ), 235 (59%) with posterior instrumentation ( ii ), and 102 (26%) with additional vertebral body replacement ( iii ). The main factor for selection towards instrumentation was a higher SINS score (SINS 9 in ii , 10 in iii vs. 7 in i , p < 0.0001). Surgical complications occurred in 55 cases (14%), slightly more frequent following instrumentations (15% ii, iii vs. 8% i , p = 0.427). Reoperations were necessary in 65 cases (16%), mostly due to SSI (n = 19, 29%), local recurrence (n = 15, 23%), and hardware failure (HWF) during follow-up (n = 9, 18%, i-iii , p = 0.7853). HWF occurred significantly more frequent in cases with multisegmental metastases at the TLJ (p = 0.0002) which were treated with longer constructs (p = 0.0092). Median postoperative survival was 10 months. The occurrence of complications reduced postoperative survival drastically in all groups (p = 0.0023).
Discussion and conclusion: In this large multicentric patient cohort with TLJ metastases, the majority of patients (85%) were treated with instrumented spine surgery. The main factor for patient selection towards instrumented surgery was a higher SINS score. Long instrumentations for multisegmental disease at the TLJ were identified with higher risk for hardware-failure during follow-up. In those patients, frequent follow-up imaging is warranted. As postoperative survival is drastically reduced by the occurrence of postoperative complications, it is imperative to carefully select the individually appropriate extent of surgery in order to avoid postoperative complications.
Keywords: Spinal metastasis; Spinal oncology; Spine instrumentation; Thoracolumbar junction; surgical indication.
© 2025 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
