

Polygenic score integrating neurodegenerative and vascular risk informs dementia risk stratification
- PMID: 40042447
- PMCID: PMC11881617
- DOI: 10.1002/alz.70014
Polygenic score integrating neurodegenerative and vascular risk informs dementia risk stratification
Abstract
Introduction: An integrative polygenic risk score (iPRS) capturing the neurodegenerative and vascular contribution to dementia could identify high-risk individuals and improve risk prediction.
Methods: We developed an iPRS for dementia (iPRS-DEM) in Europeans (aged 65+), comprising genetic risk for Alzheimer's disease (AD) and 23 vascular or neurodegenerative traits (excluding apolipoprotein E [APOE]). iPRS-DEM was evaluated across cohorts comprising older community-dwelling people (N = 3702), a multi-ancestry biobank (N = 130,797 Europeans; 105,404 non-Europeans), and dementia-free memory clinic participants (N = 2032).
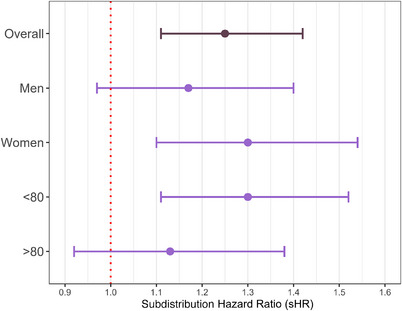
Results: iPRS-DEM was associated with dementia risk independently of APOE in the elderly (subdistribution hazard ratio [sHR]per1SD = 1.15, 95% confidence interval [CI]: 1.03 to 1.28), which generalized to Europeans (EUR-sHRper1SD = 1.28, 95% CI: 1.09 to 1.51]), East-Asians (EAS-sHRper1SD = 5.29, 95% CI: 1.43 to 34.36), and memory-clinic participants (sHRper1SD = 1.25, 95% CI: 1.11 to 1.42). Prediction was comparable to clinical risk factors in older community-dwelling people, with improved performance among memory-clinic patients. Risk stratification was enhanced by defining four genetic risk groups with iPRS-DEM and APOE ε4, reaching five-fold increased risk in APOE ε4+/iPRS-DEM+ memory-clinic participants.
Discussion: Alongside APOE ε4, iPRS-DEM may refine risk stratification for the enrichment of dementia clinical trials and prevention programs.
Highlights: iPRS-DEM reflects neurodegenerative and vascular contribution to dementia. We show iPRS-DEM captures additional dementia genetic risk beyond APOE and AD-PRS. iPRS-DEM, in combination with APOE ε4, shows promise for dementia risk stratification. Our results generalize across both population-based and memory-clinic settings. We show transportability of iPRS-DEM to East Asian ancestry.
Keywords: apolipoprotein E genotype; community‐dwelling elderly; competing risk analysis; dementia prevention; incident dementia; longitudinal study; memory clinic; multi‐ancestry biobank; polygenic risk score; transportability of PRS; vascular cognitive impairment.
© 2025 The Author(s). Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
The authors of this manuscript have no competing interests to declare. Author disclosures are available in the Supporting Information.
Figures




References
-
- Gladman JT, Corriveau RA, Debette S, et al. Vascular contributions to cognitive impairment and dementia: research consortia that focus on etiology and treatable targets to lessen the burden of dementia worldwide. Alzheimers Dement Transl Res Clin Interv. 2019;5:789‐796. doi:10.1016/j.trci.2019.09.017 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- FCS2009-2012/Fondation Plan Alzheimer
- P30AG021342/NH/NIH HHS/United States
- Conseils Régionaux of Aquitaine and Bourgogne
- Prix Fondation Claude Pompidou
- Prix NRJ-neurosciences Académie des Sciences
- Mutuelle Générale de l'Education Nationale (MGEN)
- Prix Burrus, Fondation pour la Recherche Médicale
- DGRI 2020-2024/French Ministry of Research
- 17-EURE-0019/French Investments for the Future program
- Fondation de France
- 11-LABX-0009/French National Research Agency
- R01HG010001/NH/NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- Direction Générale de la Santé
- T32 AG019134/AG/NIA NIH HHS/United States
- ANR-23-IAHU-0001/France 2030 IHU3
- Ministry of Research-INSERM Programme "Cohortes et collections de données biologiques"
- European Union's Horizon 2020 research and innovation programme under grant agreement No 754517
- P30 AG021342/AG/NIA NIH HHS/United States
- Caisse Nationale Maladie des Travailleurs Salariés
- Fondation pour la Recherche Médicale
- 32AG019134/NH/NIH HHS/United States
- Fondation Claude Pompidou
- Institut de la Longévité
- ANR-18-RHUS-0002/French National Research Agency
- EU Joint Programme - Neurodegenerative Disease Research (BRIDGET project)
- Plan Maladies Neurodégénératives
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
