

Artificial intelligence for the detection of airway nodules in chest CT scans
- PMID: 40042650
- PMCID: PMC12350537
- DOI: 10.1007/s00330-025-11468-6
Artificial intelligence for the detection of airway nodules in chest CT scans
Abstract
Objectives: Incidental airway tumors are rare and can easily be overlooked on chest CT, especially at an early stage. Therefore, we developed and assessed a deep learning-based artificial intelligence (AI) system for detecting and localizing airway nodules.
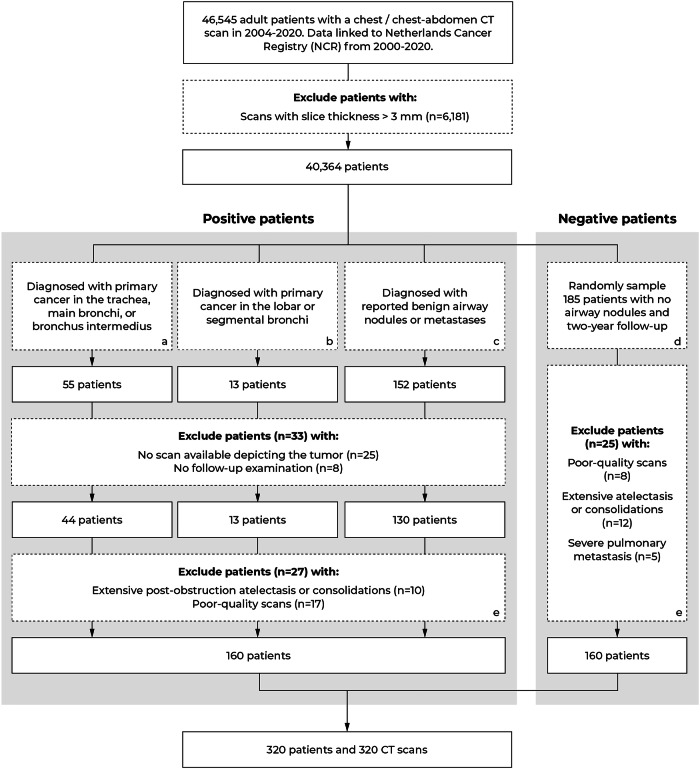
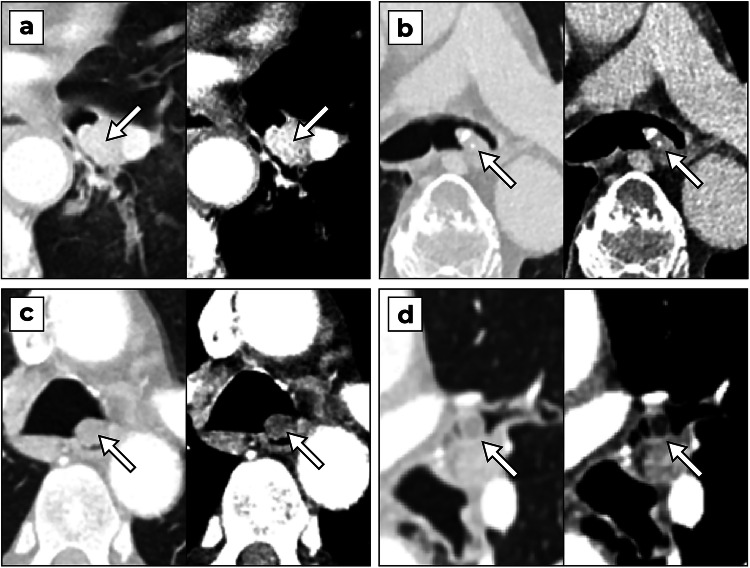
Materials and methods: At a single academic hospital, we retrospectively analyzed cancer diagnoses and radiology reports from patients who received a chest or chest-abdomen CT scan between 2004 and 2020 to find cases presenting as airway nodules. Primary cancers were verified through bronchoscopy with biopsy or cytologic testing. The malignancy status of other nodules was confirmed with bronchoscopy only or follow-up CT scans if such evidence was unavailable. An AI system was trained and evaluated with a ten-fold cross-validation procedure. The performance of the system was assessed with a free-response receiver operating characteristic curve.
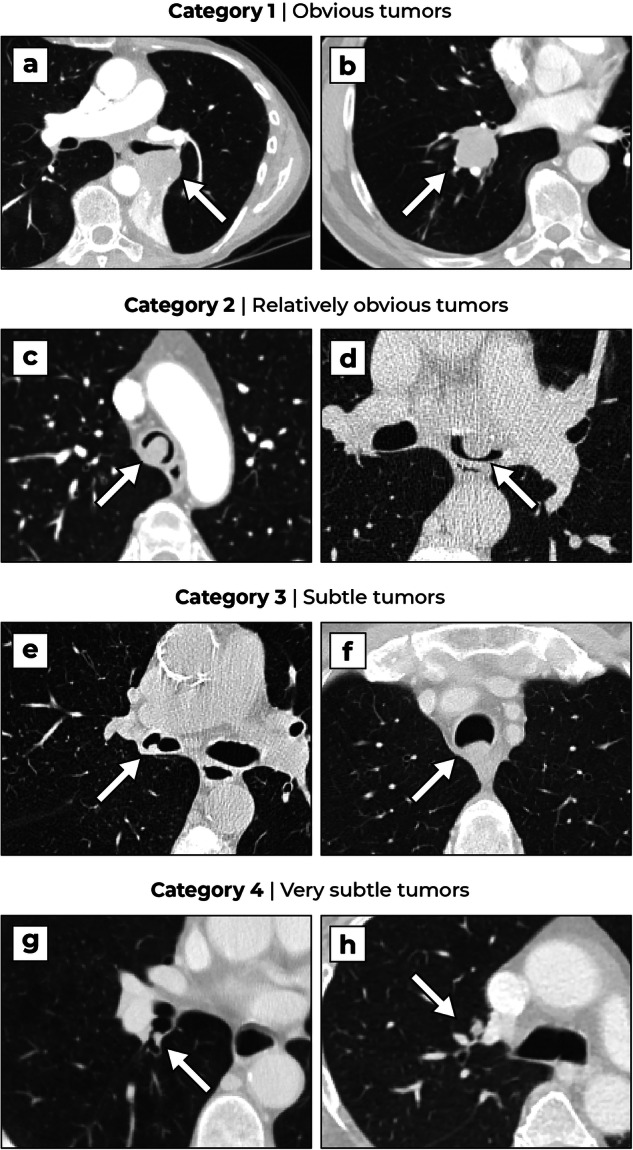
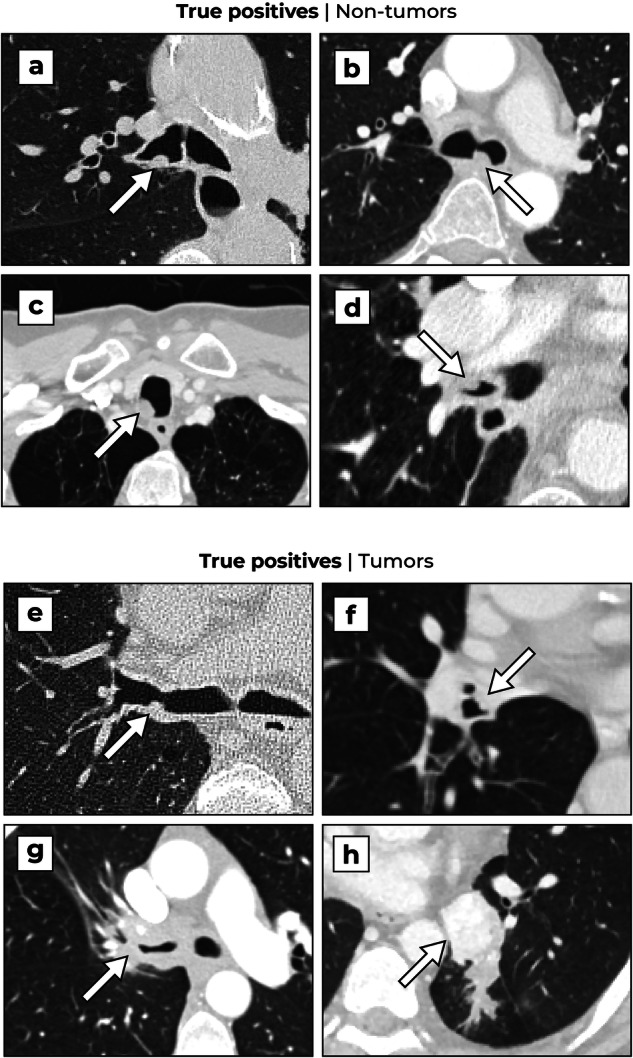
Results: We identified 160 patients with airway nodules (median age of 64 years [IQR: 54-70], 58 women) and added a random sample of 160 patients without airway nodules (median age of 60 years [IQR: 48-69], 80 women). The sensitivity of the AI system was 75.1% (95% CI: 67.6-81.6%) for detecting all nodules with an average number of false positives per scan of 0.25 in negative patients and 0.56 in positive patients. At the same operating point, the sensitivity was 79.0% (95% CI: 70.4-86.6%) for the subset of tumors. A subgroup analysis showed that the system detected the majority of subtle tumors.
Conclusion: The AI system detects most airway nodules on chest CT with an acceptable false positive rate.
Key points: Question Incidental airway tumors are rare and are susceptible to being overlooked on chest CT. Findings An AI system can detect most benign and malignant airway nodules with an acceptable false positive rate, including nodules that have very subtle features. Clinical relevance An AI system shows potential for supporting radiologists in detecting airway tumors.
Keywords: Artificial intelligence; Lung neoplasms; Thorax; Tomography (X-ray computed); Tracheal neoplasms.
© 2025. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is Colin Jacobs. Conflict of interest: The authors of this manuscript declare relationships with the following companies: B.v.G. is a shareholder and co-founder of Thirona. He reports no other relationships that are related to the subject matter of the article. M.P. receives grants from Canon Medical Systems, Siemens Healthineers; royalties from Mevis Medical Solutions; payment for lectures from Canon Medical Systems, Siemens Healthineers. The host institution of M.P. is a minority shareholder in Thirona. He reports no other relationships that are related to the subject matter of the article. The host institution of C.J. receives research grants and royalties from MeVis Medical Solutions, Bremen, Germany, and payment for lectures from Canon Medical Systems. C.J. is a collaborator in a public-private research project where Radboudumc collaborates with Philips Medical Systems (Best, the Netherlands). C.J. is a member of the Scientific Editorial Board for European Radiology (section: Imaging Informatics and Artificial Intelligence). He has not taken part in the selection or review processes for this article. He reports no other relationships that are related to the subject matter of the article. The remaining authors declare no conflicts of interest. Statistics and biometry: No complex statistical methods were necessary for this paper. Informed consent: Written informed consent was waived by the Institutional Review Board. Ethical approval: Institutional Review Board approval was obtained. Study subjects or cohorts overlap: Not applicable. Methodology: Retrospective Experimental Performed at one institution
Figures


References
-
- Honings J, van Dijck JAAM, Verhagen AFTM, van der Heijden HFM, Marres HAM (2007) Incidence and treatment of tracheal cancer: a nationwide study in the Netherlands. Ann Surg Oncol 14:968–976. 10.1245/s10434-006-9229-z - PubMed
-
- Girvin F, Phan A, Steinberger S et al (2023) Malignant and benign tracheobronchial neoplasms: comprehensive review with radiologic, bronchoscopic, and pathologic correlation. Radiographics 10.1148/RG.230045 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
