

Incidence of acute kidney injury-associated mortality in hospitalized children: a systematic review and meta-analysis
- PMID: 40045255
- PMCID: PMC11883935
- DOI: 10.1186/s12882-025-04033-2
Incidence of acute kidney injury-associated mortality in hospitalized children: a systematic review and meta-analysis
Abstract
Background: Acute kidney injury (AKI) is a significant health concern in hospitalized children and is associated with increased mortality. However, the true burden of AKI-associated mortality in pediatric populations remains unclear.
Objective: To determine the pooled incidence of mortality independently associated with AKI in hospitalized children globally.
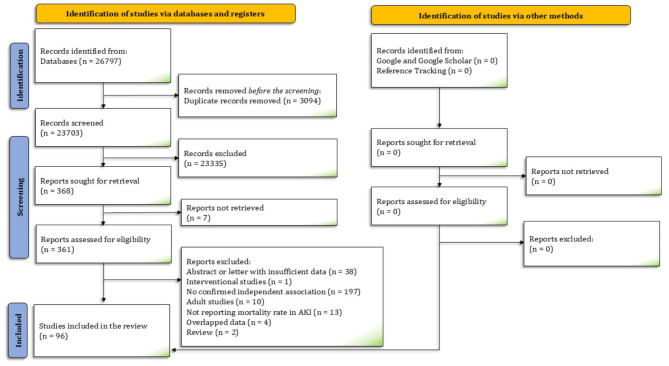
Data sources: Medline and Embase were searched for studies published by March 2024.
Study eligibility criteria: The inclusion criteria encompassed observational studies involving hospitalized pediatric patients (< 18 years old) with AKI. Only studies that identified AKI as an independent risk factor for increased mortality in multivariate analysis were considered.
Study appraisal and synthesis methods: Studies with at least 100 AKI patients were included in the meta-analysis. Two authors extracted data on the study and patients' characteristics and mortality across AKI stages and assessed the risk of bias. We used a random-effects meta-analysis to generate pooled estimates of mortality.
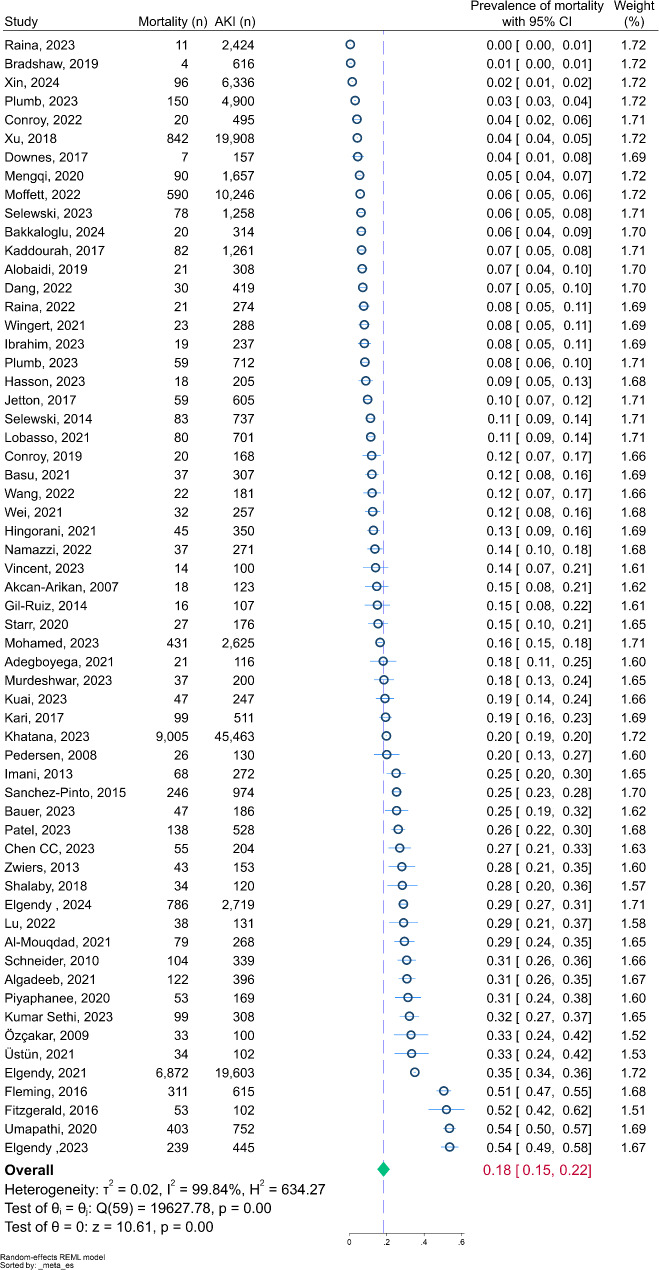
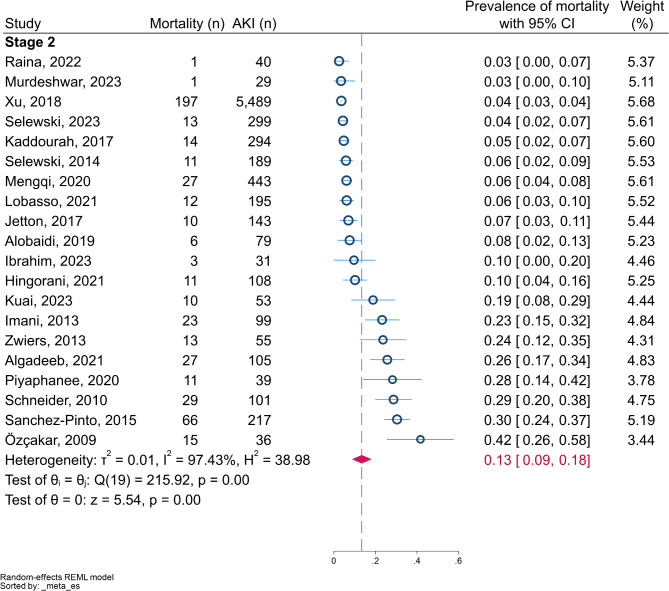
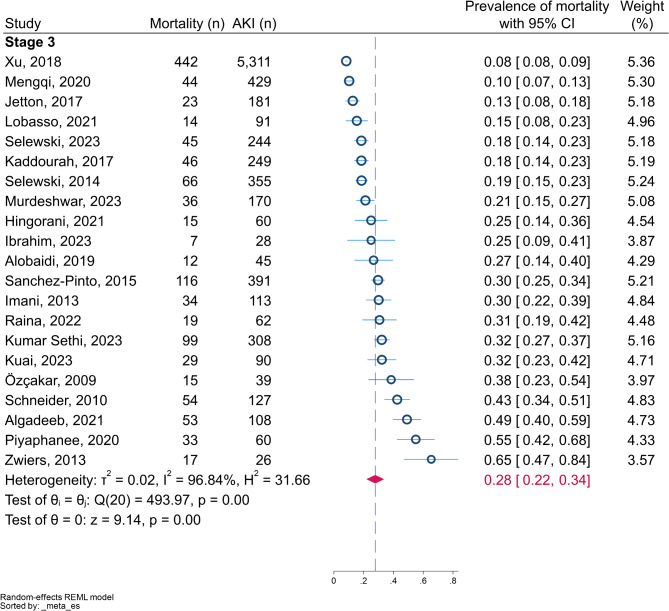
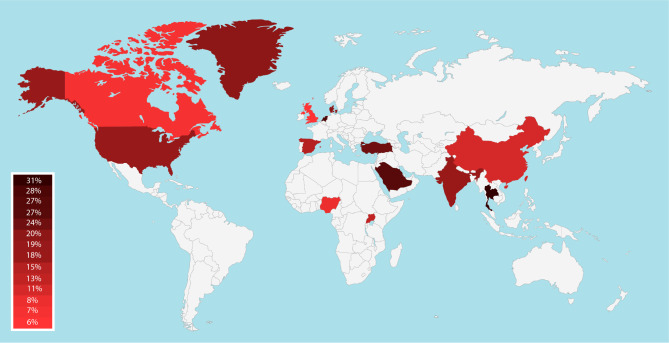
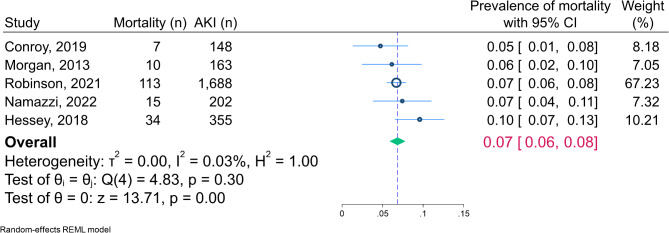
Results: Analysis of 60 studies including 133,876 children with AKI revealed a pooled in-hospital mortality rate of 18.27% (95% CI: 14.89, 21.65). Mortality increased with AKI severity; 8.19% in stage 1, 13.44% in stage 2, and 27.78% in stage 3. Subgroup analyses showed no significant differences across geographical regions, income levels, or AKI definition criteria. The pooled post-discharge mortality rate was 6.84% (95% CI: 5.86, 7.82) in a 1-9-year follow-up period.
Conclusions: This meta-analysis demonstrates a substantial global burden of AKI-associated mortality in hospitalized children, with higher mortality rates in more severe AKI stages. These findings highlight the critical need for early detection and intervention strategies in pediatric AKI management.
Clinical trial number: Not applicable.
Keywords: Acute kidney failures; Acute kidney injuries; Acute renal injury; Cause of death; Child mortality; Child, preschool; Fetal outcome; Hospital mortality; Infant; Infant, newborn.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Meena J, Mathew G, Kumar J, Chanchlani R. Incidence of acute kidney injury in hospitalized children: A Meta-analysis. Pediatrics. 2023;151(2). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
