

Multicentre, real-world data of next-generation computer-assisted vacuum aspiration thrombectomy in acute pulmonary embolism
- PMID: 40045310
- PMCID: PMC11883934
- DOI: 10.1186/s12931-025-03162-4
Multicentre, real-world data of next-generation computer-assisted vacuum aspiration thrombectomy in acute pulmonary embolism
Abstract
Background: Data on interventional treatment of intermediate-high (and high-risk pulmonary embolism (PE) are limited. The authors sought to evaluate the safety and efficacy of catheter-directed mechanical aspiration thrombectomy (CDMT) in a real-world PE patient population.
Methods: This multicenter, prospective registry enrolled PE patients treated with CDMT using the Lightning 12 System. The primary safety endpoints included in-hospital all-cause mortality, procedure-related major bleeding, clinical deterioration, or bailout to another strategy. The primary efficacy outcomes included the reduction of pulmonary arterial pressures and change in the right-to-left ventricular (RV/LV) ratio 48 h after the CDMT. Multivariate regression analyzed characteristics associated with RV/LV improvement.
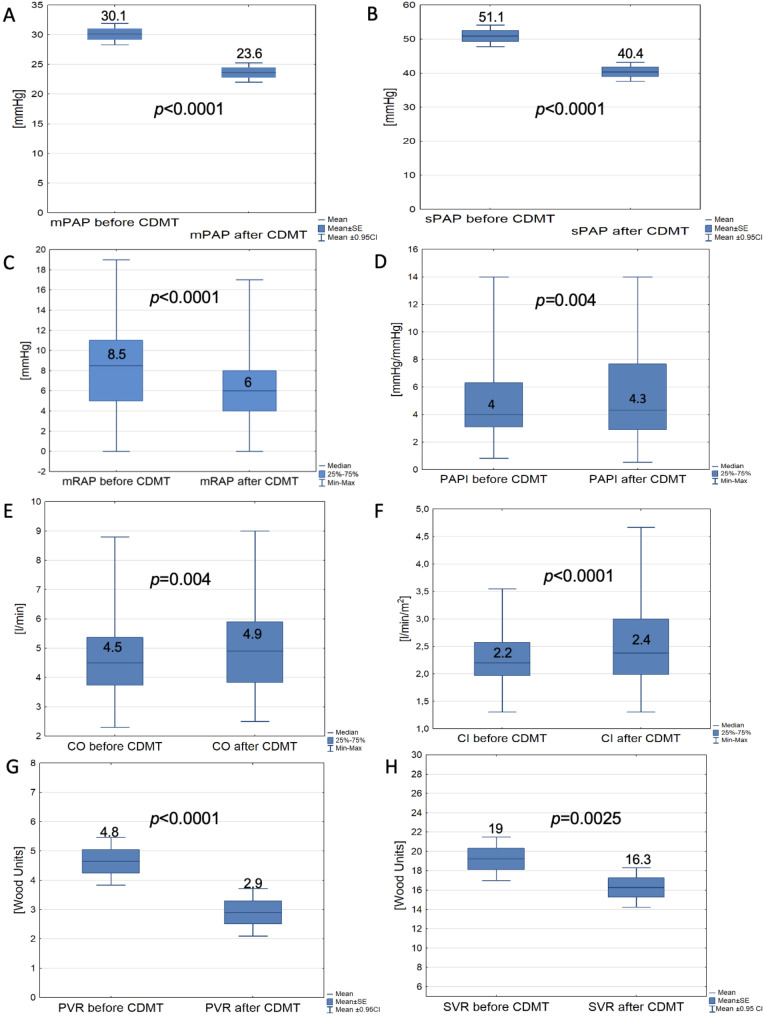
Results: Our analysis included 150 patients, 72% with intermediate-high PE and 28% with high-risk PE. Systemic thrombolysis was contraindicated in 33.3%, whereas in 4% it failed. There were 2% intraprocedural deaths (1.3% due to RV failure and 0.7% due to massive interstitial bleeding), with no more deaths during follow-up. In 0.7%, CDMT was converted to open surgery, and in 0.7%, bailout systemic thrombolysis and extracorporeal oxygenation support. Major bleedings occurred in 1.3% within 48 h post CDMT. Immediate hemodynamic improvements included a mean 11.3±10 mmHg (22.1%) drop in systolic pulmonary arterial pressure (p < 0.0001) and a median 0.33 (0.25-0.45), (25.2%) drop in RV/LV ratio (p < 0.0001 for paired values), CONCLUSIONS: Aspiration thrombectomy with the Lightning 12 system characterizes an acceptable safety profile, substantial improvements in hemodynamic outcomes, and low mortality for patients with intermediate-high and high-risk PE.
Trial registration: NCT04879069 - date of registration 04.05.2021.
Keywords: High-risk catheter-directed mechanical thrombectomy; Intermediate-high risk; Percutaneous thrombectomy; Pulmonary embolism.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the bioethics committee of the coordinating center (Poznan University of Medical Sciences Bioethics Committee; approval number 271/2021). The study was also registered at ClinicalTrials.gov (NCT04879069). All patients signed informed consent. Consent for publication: The authors affirm that human research participants provided informed consent for the anonymized data publication. Competing interests: The authors declare no competing interests.
Figures

References
-
- Bangalore S, Horowitz JM, Beam D, Jaber WA, Khandhar S, Toma C, Weinberg MD, Mina B. Prevalence and predictors of cardiogenic shock in Intermediate-Risk pulmonary embolism: insights from the FLASH registry. JACC Cardiovasc Interv. 2023;16:958–72. - PubMed
-
- Pruszczyk P, Klok FA, Kucher N, et al. Percutaneous treatment options for acute pulmonary embolism: a clinical consensus statement by the ESC working group on pulmonary circulation and right ventricular function and the European association of percutaneous cardiovascular interventions. EuroIntervention. 2022;18:e623–38. - PMC - PubMed
-
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European respiratory society (ERS). Eur Heart J. 2020;41:543–603. - PubMed
-
- Kopeć G, Araszkiewicz A, Kurzyna M, et al. Role of catheter-directed therapies in the treatment of acute pulmonary embolism. Expert opinion of the Polish PERT initiative, working group on pulmonary circulation, association of cardiovascular interventions, and association of intensive cardiac care of the Polish cardiac society. Kardiol Pol. 2023;81:423–40. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
