

Financial Rewards for Smoking Cessation During Pregnancy and Birth Weight: A Meta-Analysis
- PMID: 40048164
- PMCID: PMC11886724
- DOI: 10.1001/jamanetworkopen.2025.0214
Financial Rewards for Smoking Cessation During Pregnancy and Birth Weight: A Meta-Analysis
Abstract
Importance: Offering pregnant women financial rewards to stop smoking is associated with a more than 2-fold increase in smoking cessation and is cost-effective; however, it is possible that the association is the result of gaming of the outcome measure (eg, not smoking for 24 hours before outcome measurement using a carbon monoxide breath test). Birth weight is an outcome measure that is independent of the rewards process.
Objective: To examine birth weight change associated with offering financial rewards for smoking cessation to pregnant women, and to estimate the average expected birth weight change for neonates born to those who quit smoking because of the rewards.
Data sources: Medline, American Psychological Association PsycInfo, Embase, Cochrane (the Cochrane Central Register of Controlled Trials, the Cochrane Tobacco Addiction Group Specialized Register, and the Cochrane Database of Systematic Reviews), and PubMed were searched from their inception until December 5, 2023, for published reports of trials of incentives for abstinence from substance use among pregnant women.
Study selection: Only trials using an experimental design allowing treatment effects to be attributed to the reward intervention were included. For this review update, potentially relevant studies retrieved were screened by a reviewer.
Data extraction and synthesis: Data were pooled using both fixed-effects and random-effects models. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was followed.
Main outcomes and measures: The primary outcomes were mean (SD) birth weight, birth weight for gestational age z score, and numbers of newborns with low birth weight (<2.5 kg) and who were small for gestational age (<10th percentile).
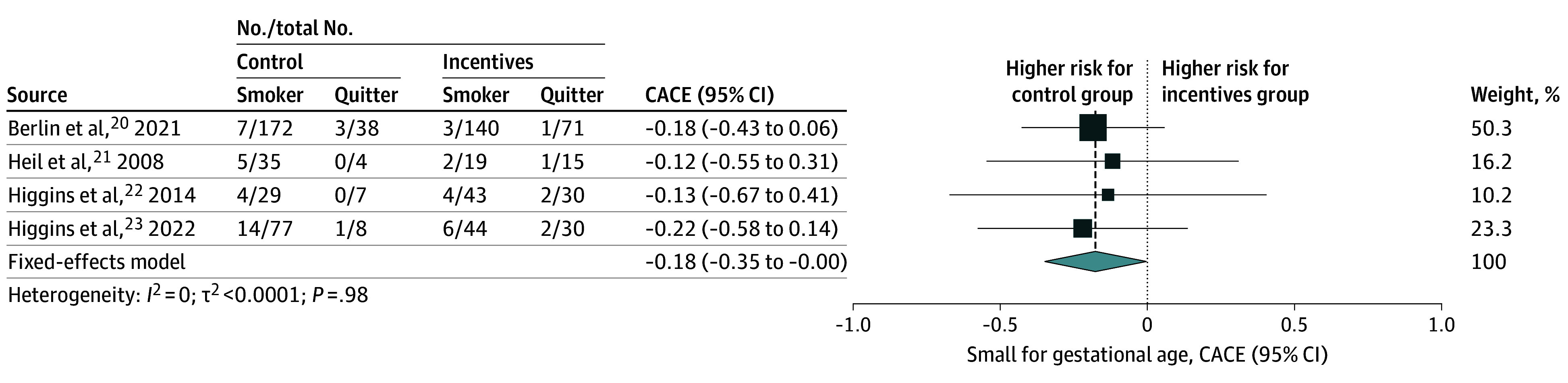
Results: Fixed-effects intention-to-treat analysis including 8 trials (2351 participants)-2 trials from the UK (1475 participants), 1 trial from France (407 participants), and 5 trials from the US (469 participants)-estimated a statistically significant mean 46.30 g (95% CI, 0.05 to 92.60 g) birth weight increase associated with adding financial rewards for smoking cessation. Complier average causal effects analysis (2239 participants) estimated a mean 206.00 g (95% CI, -69.12 to 481.14 g) increase for neonates born to smokers who quit because of rewards, but the increase was not statistically significant. There was no association with low birth weight or birth weight adjusted for gestational age, although fewer neonates were born small for gestational age, particularly if cessation was associated with rewards (complier average causal effects risk difference -17.70%; 95% CI, -34.90% to -0.42%).
Conclusions and relevance: In this meta-analysis, neonates were significantly heavier when pregnant women were offered the addition of financial rewards contingent on smoking cessation, supporting the effectiveness and, therefore, cost-effectiveness of financial rewards in this health care setting.
Conflict of interest statement
Figures



Comment in
- doi: 10.1001/jamanetworkopen.2025.0247
References
-
- US Department of Health and Human Services . A Report of the Surgeon General. Highlights: overview of finding regarding reproductive health. 2010. Accessed December 8, 2024. https://stacks.cdc.gov/pdfjs/web/viewer.html?file=https://stacks.cdc.gov...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
