

Large-Scale Plasma Proteomics to Profile Pathways and Prognosis of Chronic Pain
- PMID: 40048323
- PMCID: PMC12021123
- DOI: 10.1002/advs.202410160
Large-Scale Plasma Proteomics to Profile Pathways and Prognosis of Chronic Pain
Abstract
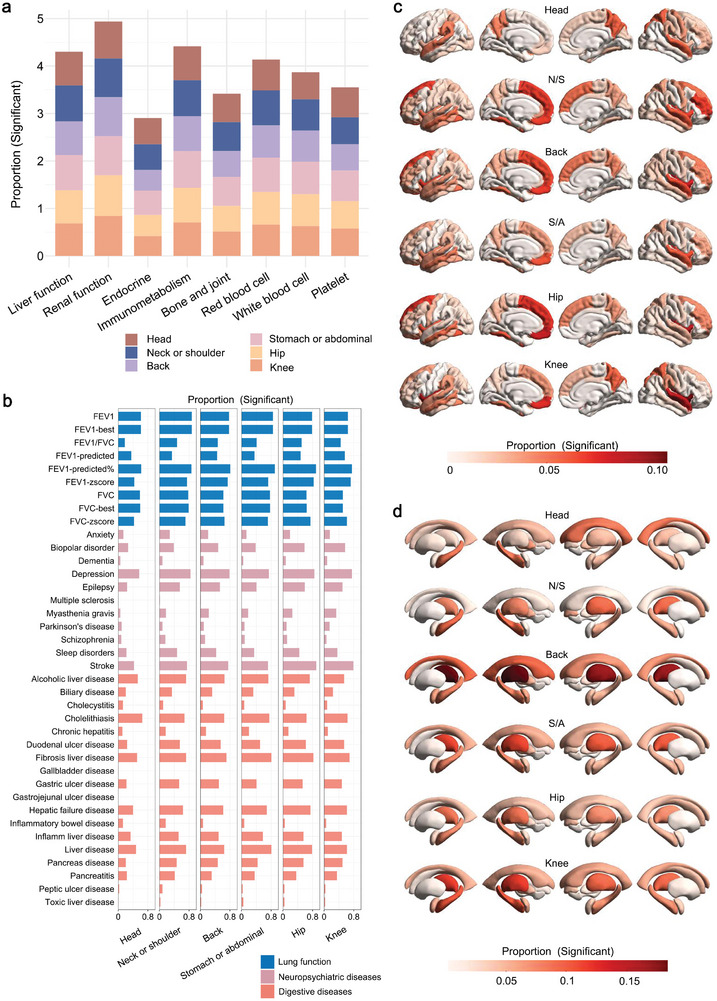
While increasing peripheral mechanisms related to chronic pain, the plasma proteomics profile associated with it and its prognosis remains elusive. This study utilizes 2923 plasma proteins and chronic pain of 51 644 participants from UK Biobank and finds 474 proteins linked to chronic pain in six sites: head, neck or shoulder, back, stomach or abdominal, hip, and knee, with 11 proteins sharing across pain sites. The identified proteins are largely enriched in immune and metabolic pathways and highly expressed in tissues like lungs and small intestines. Phenome-wide analysis highlights the significance of pain-related proteome on diverse facets of human health, and in-depth Mendelian randomization validates 10 proteins (CD302, RARRES2, TNFRSF1B, BTN2A1, TNFRSF9, COL18A1, TNF, CD74, TNFRSF4, and BTN2A1) as markers of chronic pain. Furthermore, protein sets capable of classifying pain patients and healthy participants, particularly performing best in hip pain (area under curve, AUC = 0.725), are identified. Interestingly, the prediction of pain spreading over ten years achieves an AUC of 0.715, with leptin identified as a crucial predictor. This study delineates proteins associated with various pain conditions and identifies proteins capable of classifying pain and predicting pain spreading, offering benefits for both research and clinical practice.
Keywords: Mendelian randomization; UK Biobank; chronic pain; plasma proteomic; prediction.
© 2025 The Author(s). Advanced Science published by Wiley‐VCH GmbH.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
MeSH terms
Substances
Grants and funding
- 2023YFC3605400/National Key R&D Program of China
- 82472055/National Natural Science Foundation of China
- 82071201/National Natural Science Foundation of China
- 82271471/National Natural Science Foundation of China
- 92249305/National Natural Science Foundation of China
- 2022ZD0211600/The STI2030-Major Projects
- 2023SHZDZX02/Shanghai Municipal Science and Technology Major Project
- 2018SHZDZX01/Shanghai Municipal Science and Technology Major Project
- 2022QD002/Research Start-up Fund of Huashan Hospital
- 3030277001/Excellence 2025 Talent Cultivation Program at Fudan University
- 23XD1420400/Program of Shanghai Academic Research Leader
- B18015/The 111 Project
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous