

The effect of IL-1β inhibitor canakinumab (Ilaris®) on IL-6 production in human skeletal muscle cells
- PMID: 40048444
- PMCID: PMC11884680
- DOI: 10.1371/journal.pone.0316110
The effect of IL-1β inhibitor canakinumab (Ilaris®) on IL-6 production in human skeletal muscle cells
Abstract
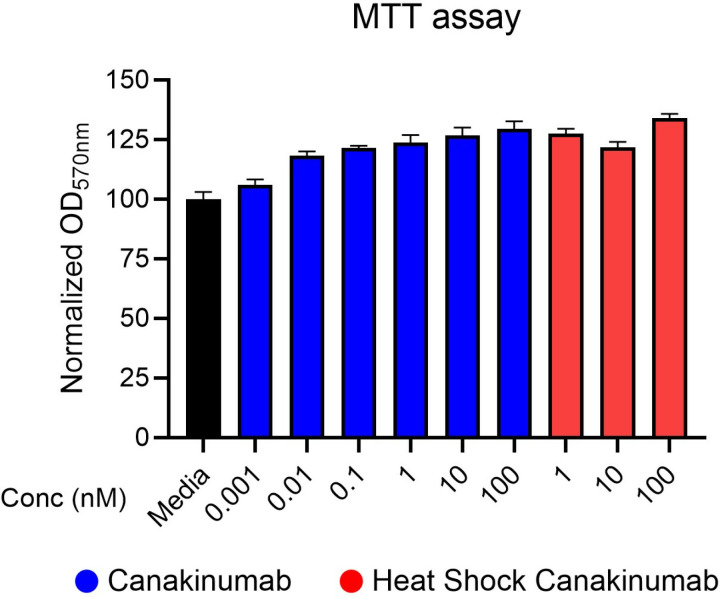
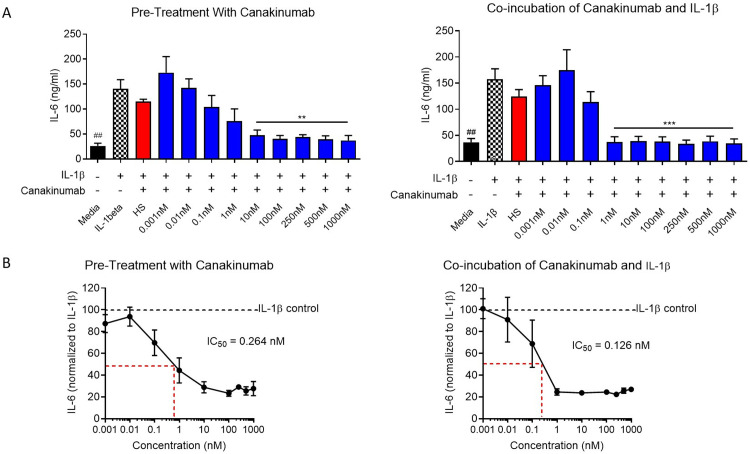
Muscle inflammation is one of the hallmarks of Duchenne muscular dystrophy (DMD). Dystrophin-deficient skeletal muscle cells produce higher levels of pro-inflammatory cytokines such as interleukin 1β (IL-1β) in response to toll-like receptor stimulation compared to normal muscle skeletal cells. IL- 1β induces the human skeletal muscle secretion of the myokine Interleukin-6 (IL-6). Here, we evaluated the effect of a human IgG1κ monoclonal antibody (canakinumab (Ilaris®)) that specifically blocks the IL-1β effect on IL-6 secretion by human skeletal muscle cells. Canakinumab is an excellent candidate for therapeutic repositioning to treat DMD because it is an FDA-approved drug to treat periodic fever syndromes and systemic juvenile idiopathic arthritis. Unlike previous generations of IL-1 inhibitors, canakinumab is highly specific for the IL-1β ligand, has a longer half-life, and does not interfere with other IL-1-activated inflammatory pathways. Following cell culture optimization and viability assays to assess toxicity, skeletal muscle cells were stimulated with IL-1β (10 ng/mL) for 48 hours in the presence of nine concentrations of canakinumab ranging from 0.001 nM to 1000 nM, and IL-6 production was measured with an enzyme-linked immunosorbent assay. Pre-incubation of myoblasts with canakinumab before IL-1β-stimulation, significantly reduced IL-6 production at concentrations of 1, 10, 100, 250, and 1000 nM relative to controls, yielding an IC50 of 0.264 nM. On the other hand, co-incubation of canakinumab with IL-1β before addition to myoblasts resulted in a significant inhibition with the IC50 reducing to 0.126 nM, less than half of the previous method. Canakinumab also did not affect myotube viability at 10 nM and was also able to significantly reduce the production of IL-6, when the cells were stimulated with IL-1β (10 ng/ml). Taken together, our results show that canakinumab is a potent inhibitor of IL-1β signaling in muscle cells. These results align with previously published pre-clinical work with other IL-1 inhibitors in the mdx mouse model and support further investigation into the clinical utility of repositioning canakinumab to treat DMD.
Copyright: © 2025 Cordeiro-Santanach et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist. EPH and KN are cofounders of AGADA Biosciences Inc. ACS, FM, MCP, KU, JR, JW, WW and PE are employees of AGADA Biosciences Inc. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures




References
-
- Systemic Inflammation in Duchenne Muscular Dystrophy: Association with Muscle Function and Nutritional Status - Cruz-Guzmán - 2015 - BioMed Research International - Wiley Online Library [Internet]. [cited 2024 Oct 11]. Available from: https://onlinelibrary.wiley.com/doi/10.1155/2015/891972 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
