

Advances in acute respiratory distress syndrome: focusing on heterogeneity, pathophysiology, and therapeutic strategies
- PMID: 40050633
- PMCID: PMC11885678
- DOI: 10.1038/s41392-025-02127-9
Advances in acute respiratory distress syndrome: focusing on heterogeneity, pathophysiology, and therapeutic strategies
Abstract
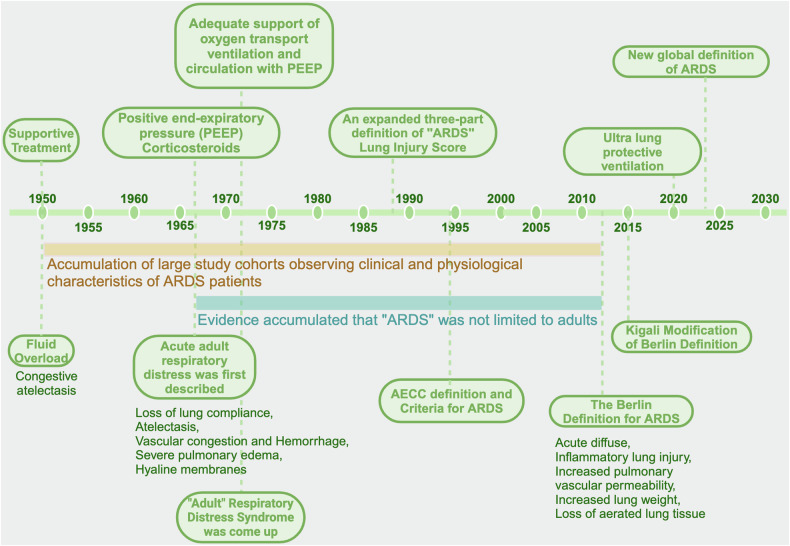
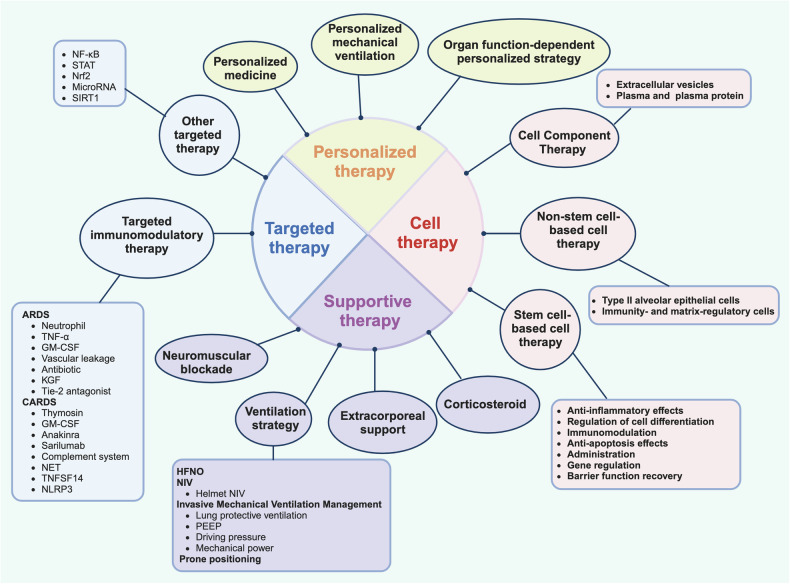
In recent years, the incidence of acute respiratory distress syndrome (ARDS) has been gradually increasing. Despite advances in supportive care, ARDS remains a significant cause of morbidity and mortality in critically ill patients. ARDS is characterized by acute hypoxaemic respiratory failure with diffuse pulmonary inflammation and bilateral edema due to excessive alveolocapillary permeability in patients with non-cardiogenic pulmonary diseases. Over the past seven decades, our understanding of the pathology and clinical characteristics of ARDS has evolved significantly, yet it remains an area of active research and discovery. ARDS is highly heterogeneous, including diverse pathological causes, clinical presentations, and treatment responses, presenting a significant challenge for clinicians and researchers. In this review, we comprehensively discuss the latest advancements in ARDS research, focusing on its heterogeneity, pathophysiological mechanisms, and emerging therapeutic approaches, such as cellular therapy, immunotherapy, and targeted therapy. Moreover, we also examine the pathological characteristics of COVID-19-related ARDS and discuss the corresponding therapeutic approaches. In the face of challenges posed by ARDS heterogeneity, recent advancements offer hope for improved patient outcomes. Further research is essential to translate these findings into effective clinical interventions and personalized treatment approaches for ARDS, ultimately leading to better outcomes for patients suffering from ARDS.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare that they have no competing interests. Yu Cao is the editorial board member of Signal Transduction and Targeted Therapy, but she has not been involved in the process of manuscript handling.
Figures

References
-
- Jenkins, M. T., Jones, R. F., Wilson, B. & Moyer, C. A. Congestive atelectasis; a complication of the intravenous infusion of fluids. Trans. Meet. Am. Surg. Assoc. Am. Surg. Assoc.68, 7–27 (1950). - PubMed
-
- Ashbaugh, D. G., Bigelow, D. B., Petty, T. L. & Levine, B. E. Acute respiratory distress in adults. Lancet2, 319–323 (1967). - PubMed
-
- Petty, T. L. & Ashbaugh, D. G. The adult respiratory distress syndrome. Clinical features, factors influencing prognosis and principles of management. Chest60, 233–239 (1971). - PubMed
-
- Murray, J. F., Matthay, M. A., Luce, J. M. & Flick, M. R. An expanded definition of the adult respiratory distress syndrome. Am. Rev. Respir. Dis.138, 720–723 (1988). - PubMed
-
- Baden, M. et al. A controlled trial of hydrocortisone therapy in infants with respiratory distress syndrome. Pediatrics50, 526–534 (1972). - PubMed
Publication types
MeSH terms
Grants and funding
- 82241060/National Natural Science Foundation of China (National Science Foundation of China)
- 82272241/National Natural Science Foundation of China (National Science Foundation of China)
- 82402574/National Natural Science Foundation of China (National Science Foundation of China)
- 82270392/National Natural Science Foundation of China (National Science Foundation of China)
- 2023M732462/China Postdoctoral Science Foundation
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
