

Repurposing pitavastatin and atorvastatin to overcome chemoresistance of metastatic colorectal cancer under high glucose conditions
- PMID: 40050889
- PMCID: PMC11887183
- DOI: 10.1186/s12935-025-03712-2
Repurposing pitavastatin and atorvastatin to overcome chemoresistance of metastatic colorectal cancer under high glucose conditions
Abstract
Background: Colorectal cancer (CRC) poses a significant clinical challenge because of drug resistance, which can adversely impact patient outcomes. Recent research has shown that abnormalities within the tumor microenvironment, especially hyperglycemia, play a crucial role in promoting metastasis and chemoresistance, and thereby determine the overall prognosis of patients with advanced CRC.
Methods: This study employs data mining and consensus molecular subtype (CMS) techniques to identify pitavastatin and atorvastatin as potential agents for targeting high glucose-induced drug resistance in advanced CRC cells. CRC cells maintained under either low or high glucose conditions were established and utilized to assess the cytotoxic effects of pitavastatin and atorvastatin, both with and without 5-fluorouracil (5-FU). CRC 3D spheroids cultured were also included to demonstrate the anti-drug resistance of pitavastatin and atorvastatin.
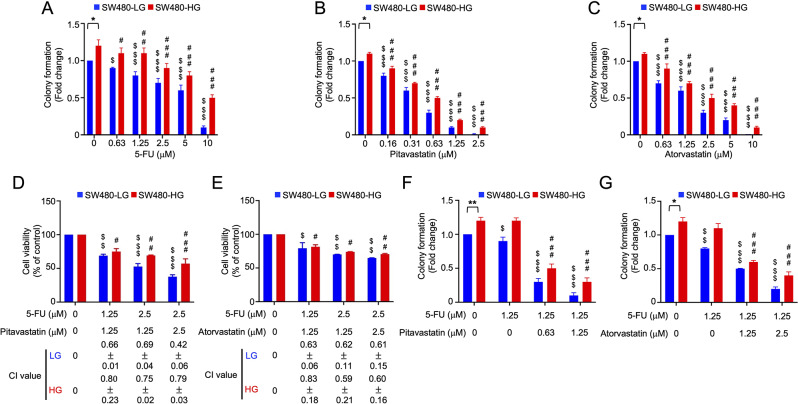
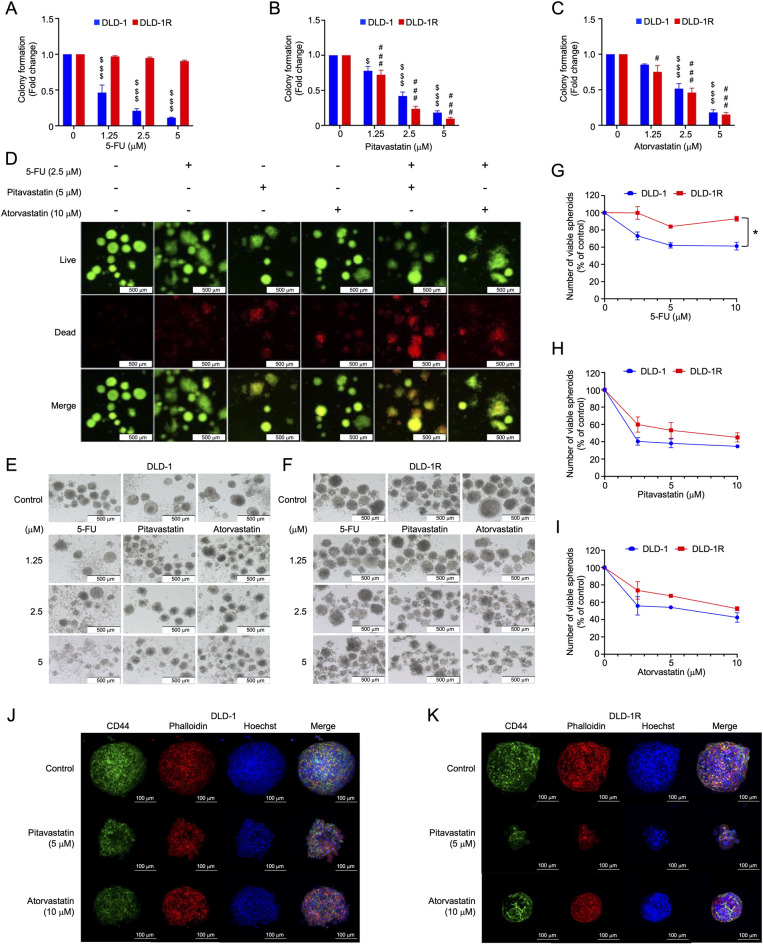
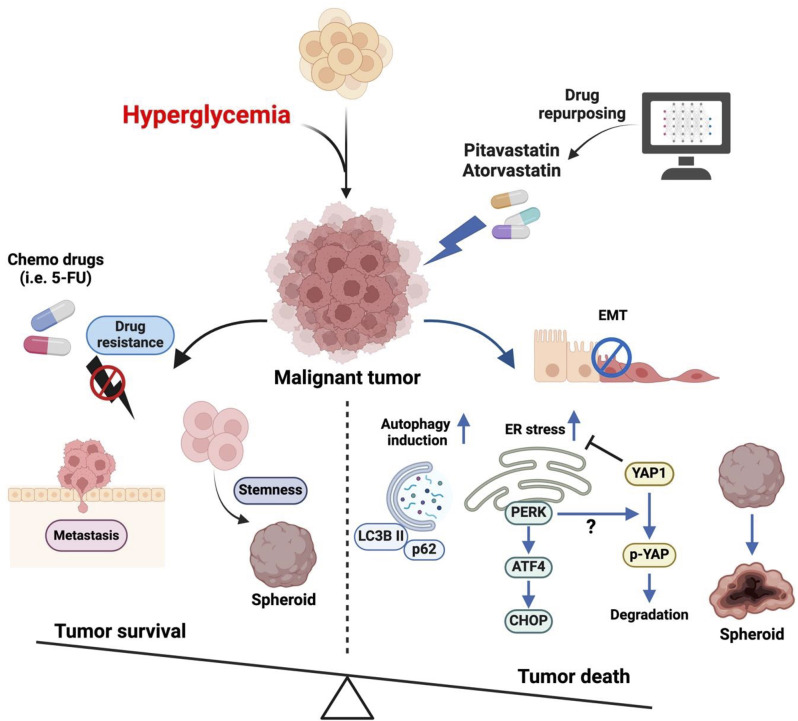
Results: A bioinformatics analysis identified pitavastatin and atorvastatin as promising drug candidates. The CMS4 CRC cell line SW480 (SW480-HG) was established and cultured under high glucose conditions to simulate hyperglycemia-induced drug resistance and metastasis in CRC patients. Pitavastatin and atorvastatin could inhibit cell proliferation and 3D spheroid formation of CMS4 CRC cells under high glucose conditions. In addition, both pitavastatin and atorvastatin can synergistically promote the 5-FU-mediated cytotoxic effect and inhibit the growth of 5-FU-resistant CRC cells. Mechanistically, pitavastatin and atorvastatin can induce apoptosis and synergistically promote the 5-FU-mediated cytotoxic effect by activating autophagy, as well as the PERK/ATF4/CHOP signaling pathway while decreasing YAP expression.
Conclusion: This study highlights the biomarker-guided precision medicine strategy for drug repurposing. Pitavastatin and atorvastatin could be used to assist in the treatment of advanced CRC, particularly with CMS4 subtype CRC patients who also suffer from hyperglycemia. Pitavastatin, with an achievable dosage used for clinical interventions, is highly recommended for a novel CRC therapeutic strategy.
Keywords: Atorvastatin; Colorectal cancer; Consensus molecular subtype; Drug resistance; Hyperglycemia; Pitavastatin.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: All authors have participated in the study and consented to publication. Competing interests: The authors declare no competing interests.
Figures




References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Kasi PM, Shahjehan F, Cochuyt JJ, Li Z, Colibaseanu DT, Merchea A. Rising proportion of young individuals with rectal and Colon cancer. Clin Colorectal Cancer. 2019;18(1):e87–95. - PubMed
-
- Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen YJ, Ciombor KK, Cohen S, Cooper HS, Deming D, Farkas L, et al. Colon cancer, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19(3):329–59. - PubMed
-
- Miller KD, Nogueira L, Mariotto AB, Rowland JH, Yabroff KR, Alfano CM, Jemal A, Kramer JL, Siegel RL. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69(5):363–85. - PubMed
Grants and funding
- 11201-62-016/Department of Health, Taipei City Government
- TPCH-113-45/Taipei City Hospital
- MOST111-2320-B-039-019-MY3/Integrated Research Plan of the National Science and Technology Council
- NSTC 113-2321-B-A49-024/Integrated Research Plan of the National Science and Technology Council
- MOST 111-2320-B-030-008/Integrated Research Plan of the National Science and Technology Council
- MOST111-2320-B-A49-036/Integrated Research Plan of the National Science and Technology Council
- CMU111-MF-44/China Medical University, Taiwan
- MLCF_V113_A11302/Melissa Lee Cancer Foundation
- PL202108010V/Fu Jen Catholic University Hospital
- 112W31101/The Ministry of Education, Higher Education SPROUT Project for the Cancer and Immunology Research Center
LinkOut - more resources
Full Text Sources
Research Materials
