

First-in-human clinical study of an embryonic stem cell product for urea cycle disorders
- PMID: 40050977
- PMCID: PMC11887382
- DOI: 10.1186/s13287-025-04162-3
First-in-human clinical study of an embryonic stem cell product for urea cycle disorders
Abstract
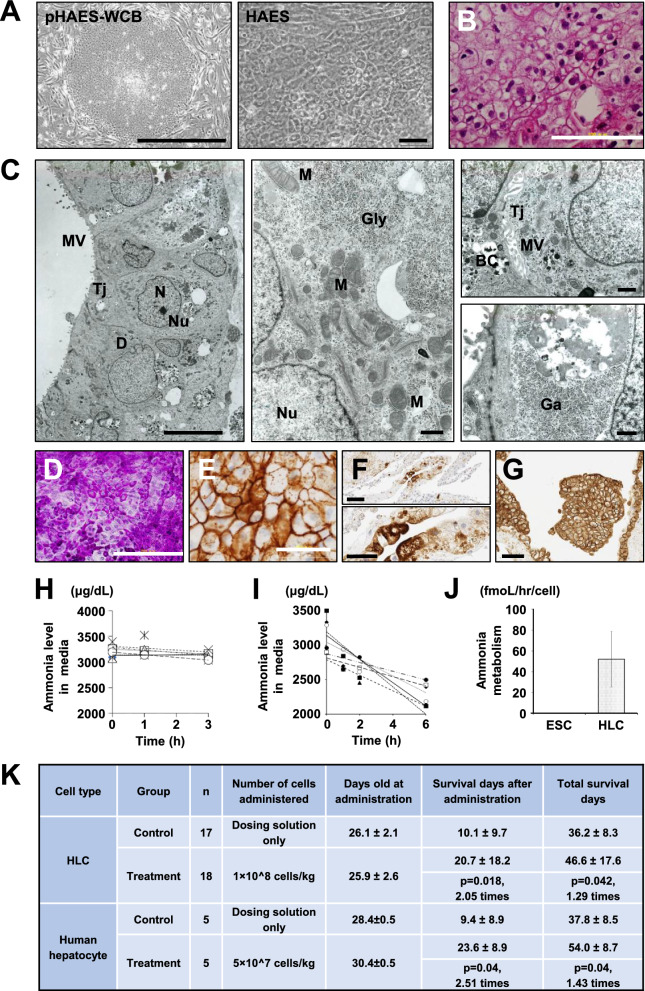
Background: This study assesses the safety and efficacy of hepatocyte-like cell (HLC) infusion therapy derived from human embryonic stem cells as bridging therapy for neonatal-onset urea cycle disorders (UCD). The research includes both preclinical and clinical evaluations to determine the feasibility of HLC infusion as a therapeutic option for safer pediatric liver transplantation.
Methods: Preclinical studies were conducted to validate the safety, biodistribution, and ammonia metabolism capabilities of HLCs using SCID mice models of UCD and extensive animal studies. In the clinical trial, five neonates with UCD received HLC infusions, intending to maintain metabolic stability and exceed a target weight of over 6 kg, which is considered necessary for safer liver transplantation.
Results: Preclinical studies demonstrated that HLCs successfully engrafted in the liver without adverse migration or tumor formation and effectively elongated survival. Clinically, all five neonates exceeded the target weight of 6 kg while maintaining metabolic stability and successfully bridging to transplantation. Post-transplantation follow-up revealed stable growth, metabolic control, and no neurological complications.
Conclusions: The combined preclinical and clinical findings support HLC infusion as a viable bridge therapy for neonates with UCD, providing metabolic support to achieve safer weight thresholds for transplantation. While promising, careful monitoring remains essential, particularly for potential complications such as thrombus formation.
Trial registration: jRCT, jRCT1090220412. Registered on 27 February 2019, https://jrct.niph.go.jp/en-latest-detail/jRCT1090220412 (originally registered in JMACCT (JMA-IIA00412)).
Keywords: Ammonia removal; Cell-based therapy; Embryonic stem cells (ESCs); Hepatocyte; Hyperammonemia; Liver transplantation; Neonatal-onset; Regenerative medicine; Urea cycle disorders (UCD).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The animal experiments were approved by The Experimental Animal Committee of the National Center for Child Health and Development Research Institute (Tokyo, JAPAN) on November 24, 2016 (study title: "The Preclinical Study of ESC-Derived Regenerative Medical Products (HAES) with Ammonia Metabolism Ability," reference number: A2016-008). The protocol of the trial was formally approved by the institutional review board of the National Center for Child Health and Development on April 28, 2018 (study title: "Clinical study of HAES transplantation in patients with neonatal onset urea cycle disorder (HAES transplantation study in patients with neonatal onset urea cycle disorder)," reference number: C29007). As the subjects of this clinical trial were neonates and infants, informed consent was obtained in accordance with ethical standards. Specifically, informed consent for participation in the trial was obtained after thoroughly explaining the study to the surrogate (parents or legal guardians). Consent for publication: Informed consent for publication in the trial was obtained after thoroughly explaining the study to the surrogate (parents or legal guardians). Competing interests: AU is a stockholder of iHaes, a biotechnology company focusing on stem cells and regenerative medicine. SE and TO are involved in manufacturing and sales for iHaes. The other authors declare that they have no conflicts of interest.
Figures



References
-
- Kasahara M, Umeshita K, Eguchi S, et al. Outcomes of pediatric liver transplantation in Japan: a report from the registry of the Japanese liver transplantation society. Transplantation. 2021;105(12):2587–95. - PubMed
-
- Mew NA, Simpson KL, Gropman AL, Lanpher BC, Chapman KA, Summar ML. Urea cycle disorders overview. In: GeneReviews® [Internet]. Seattle:University of Washington; 2017. - PubMed
-
- Fisher RA, Strom SC. Human hepatocyte transplantation: worldwide results. Transplantation. 2006;82(4):441–9. - PubMed
-
- Enosawa S, Horikawa R, Yamamoto A, et al. Hepatocyte transplantation using a living donor reduced graft in a baby with ornithine transcarbamylase deficiency: a novel source of hepatocytes. Liver Transpl. 2014;20(3):391–3. - PubMed
-
- Schwartz SD, Hubschman JP, Heilwell G, et al. Embryonic stem cell trials for macular degeneration: a preliminary report. Lancet. 2012;379(9817):713–20. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
