

Comparing methods for plasma HDV RNA quantification in bulevirtide-treated and untreated patients with HDV
- PMID: 40051411
- PMCID: PMC11883403
- DOI: 10.1016/j.jhepr.2024.101299
Comparing methods for plasma HDV RNA quantification in bulevirtide-treated and untreated patients with HDV
Abstract
Background & aims: Accurate HDV RNA quantification is crucial for diagnosis and management of chronic hepatitis delta (CHD), yet a significant variability between assays exists. We compared three methods to quantify HDV RNA levels in untreated and bulevirtide (BLV)-treated patients with CHD.
Methods: Frozen plasma from untreated and BLV-treated patients with CHD were tested in a single-center retrospective study using three different assays: Robogene 2.0 HDV RNA Quantification Kit 2.0 (Roboscreen GmbH; limit of detection [LOD] 6 IU/ml on 7500 Fast Real-Time PCR System [Applied Biosystem]), EurobioPlex HDV PCR quantitative kit (Eurobio Scientific; LOD 100 IU/m) on CFX96™ real-time PCR detection system [Bio-Rad]), and AltoStar HDV RT-PCR RUO Kit 1.5 (Altona Diagnostics; estimated LOD <10 IU/ml) on the AltoStar®AM16.
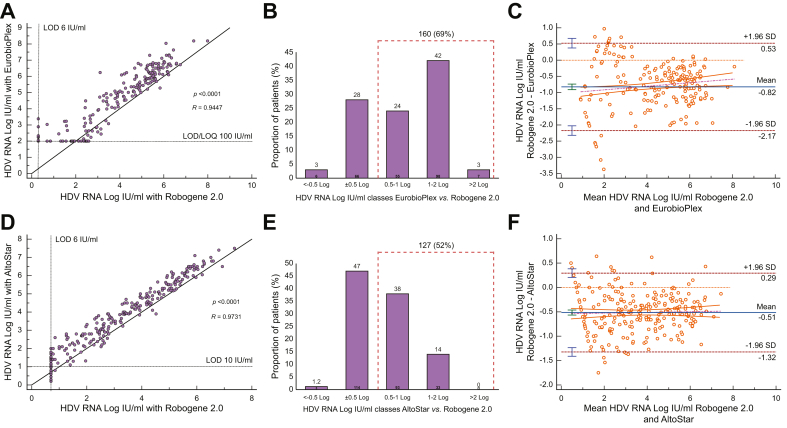
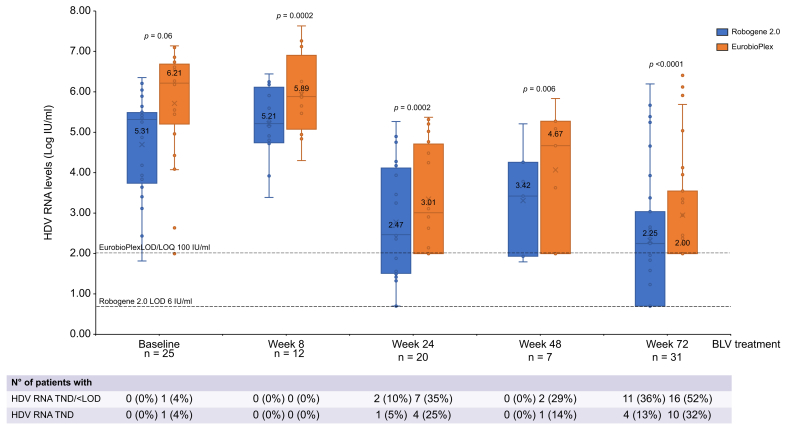
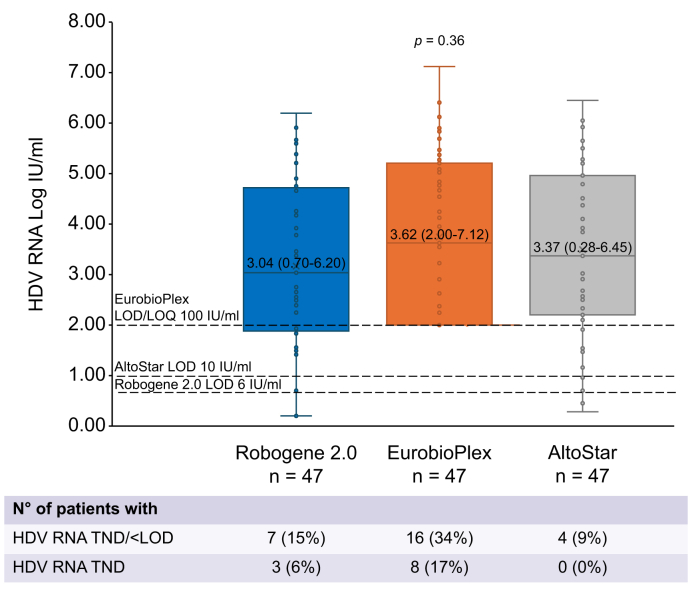
Results: Overall, 431 plasma samples from 130 patients with CHD (69 untreated and 61 BLV-treated) were studied. Compared with Robogene 2.0, EurobioPlex reported higher HDV RNA levels (3.78 [0.70-7.99] vs. 4.69 [2.00-8.19] log IU/ml, p <0.0001), with viremia higher than >0.5 log in 160 (69%). Likewise, HDV RNA levels were higher with AltoStar than with Robogene 2.0 (3.32 [0.70-7.37] vs. 3.91 [0.19-7.54] log IU/ml, p <0.0001), with AltoStar reporting HDV RNA levels >0.5 log in 127 (52%). Although virological response rates (≥2 log decline vs. baseline) at Weeks 24 (Robogene 2.0 vs. EurobioPlex and AltoStar) and 48 (Robogene 2.0 vs. AltoStar) were similar across assays, rates of HDV RNA undetectability significantly differed between the three assays at Weeks 24 and 72 (p = 0.003 and p = 0.02, respectively).
Conclusions: HDV RNA levels quantified by EurobioPlex and AltoStar were 1 and 0.5 logs higher than those quantified by Robogene 2.0, respectively. HDV RNA undetectability rates during BLV treatment were assay-dependent.
Impact and implications: Management and diagnosis of chronic hepatitis delta (CHD) require standardized tests for HDV RNA quantification. Quantification of HDV RNA is significantly influenced by the quantification method, with EurobioPlex detecting approximatively 1 log and AltoStar 0.5 log IU/ml more than Robogene 2.0, respectively. The HDV RNA undetectability rates during BLV monotherapy significantly differed among assays. These findings are of clinical relevance as patients who achieve negative viremia during BLV monotherapy might be entitled to stop therapy successfully.
Keywords: AltoStar; Antiviral therapy; Bulevirtide; Chronic hepatitis delta; EurobioPlex; HDV; HDV RNA; Nucleic acid; PCR; Robogene.
© 2024 The Authors.
Conflict of interest statement
ED is an advisory board member for AbbVie and receives speaking and teaching fees from Gilead, MSD, and AbbVie. PL is an advisor and speaker bureau for Roche Pharma/Diagnostics, Gilead Sciences, Gsk, AbbVie, Janssen, Myr, Eiger, Antios, Aligos, Vir, Grifols, Altona, and Roboscreen. The other authors have nothing to disclose. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures



References
-
- Fattovich G., Boscaro S., Noventa F., et al. Influence of hepatitis delta virus infection on progression to cirrhosis in chronic hepatitis type B. J Infect Dis. 1987;155:931–935. - PubMed
-
- Rosina F., Conoscitore P., Cuppone R., et al. Changing pattern of chronic hepatitis D in Southern Europe. Gastroenterology. 1999;117:161–166. - PubMed
-
- Wedemeyer H., Yurdaydin C., Hardtke S., et al. Peginterferon alfa-2a plus tenofovir disoproxil fumarate for hepatitis D (HIDIT-II): a randomized, placebo controlled, phase 2 trial. Lancet Infect Dis. 2019;19:275–286. - PubMed
