

CD163 detection in immune check-point inhibitors-related acute interstitial nephritis
- PMID: 40052170
- PMCID: PMC11883220
- DOI: 10.1093/ckj/sfaf009
CD163 detection in immune check-point inhibitors-related acute interstitial nephritis
Abstract
Background: Acute interstitial nephritis (AIN) is the most common renal immune-related adverse event after immune check-point inhibitors (ICI). We hypothesized that alternatively activated macrophages (CD163-M) could be involved in ICI-AIN and wished to evaluate the use of their soluble urinary form (us)CD163 as a non-invasive diagnostic marker.
Methods: CD163-M infiltrates were evaluated by both immune-histochemistry and multiplex immunofluorescence and imaging. usCD163 was detected with ELLA technology and evaluated together with urinary creatinine to be expressed as a ratio to creatinuria in ng/mmol. Clinical data were collected to perform correlations with renal function assessed by estimated glomerular filtration rate (eGFR).
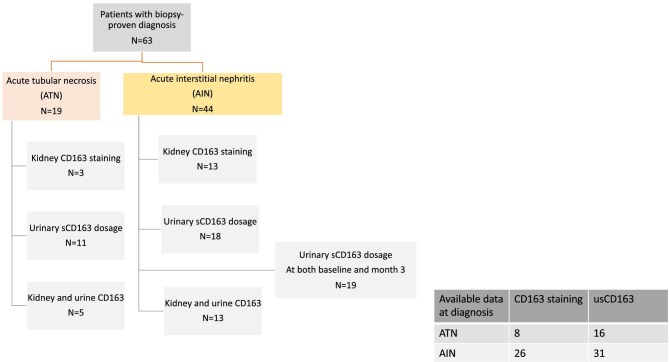
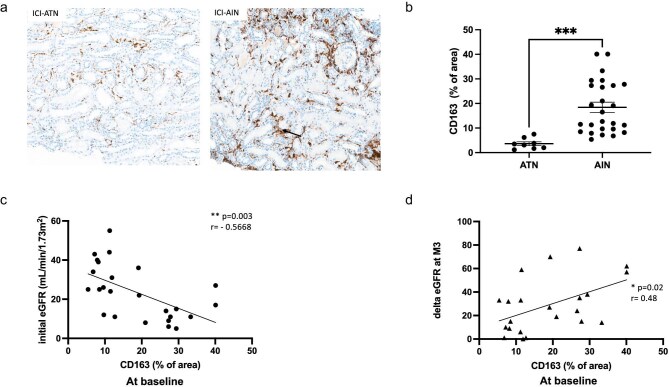
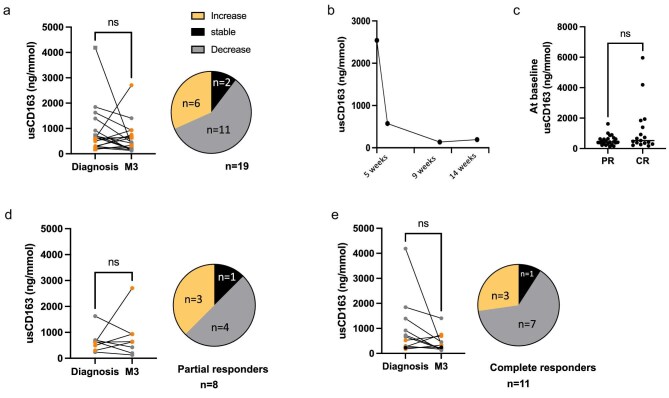
Results: A retrospective cohort of 63 ICI-exposed patients with tubular acute kidney injury profile requiring a biopsy were selected. AIN patients (n = 44) were compared to acute tubular necrosis (ATN) patients (n = 19). CD163-M staining was detectable in all ICI-AIN patients, which was significantly higher than in ATN patients (18.4% vs 3.6% of area, P = .005). CD163-M staining was restricted to the interstitial compartment. CD163-M infiltrate inversely correlated with initial eGFR (r = -0.6, P = .003), and was positively correlated with delta eGFR, reflecting a renal improvement outcome (r = 0.48; P = .02). usCD163 was well detected in urines of patients, but did not allow us to distinguish ATN from AIN patients at diagnosis. No correlation was observed, neither between usCD163 and CD163-M staining nor with renal response after 3 months of glucocorticoid tapering.
Conclusion: CD163-M are detected in ICI-AIN and correlate both with severity at diagnosis and better prognosis at 3 months. CD163-M may help us to distinguish AIN from ATN but, it does not allow us to assess ICI imputability. Although detected in urine, usCD163 is clearly not a surrogate biomarker for AIN diagnosis.
Keywords: CD163; alternatively activated macrophage; immune check-point inhibitors acute interstitial nephritis ICI-AIN; urinary soluble usCD163.
© The Author(s) 2025. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
Dr Belliere Julie : Employer: Centre hospitalier universitaire de Toulouse; Symposia: Astellas, Sandoz, CSL-Vifor, Sanofi, Congrès Colloques Convention, AstraZeneca.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
