

Harnessing the Plasma Proteome to Predict Mortality in Heart Failure Subpopulations
- PMID: 40052265
- PMCID: PMC11995852
- DOI: 10.1161/CIRCHEARTFAILURE.123.011208
Harnessing the Plasma Proteome to Predict Mortality in Heart Failure Subpopulations
Abstract
Background: We derived and validated proteomic risk scores (PRSs) for heart failure (HF) prognosis that provide absolute risk estimates for all-cause mortality within 1 year.
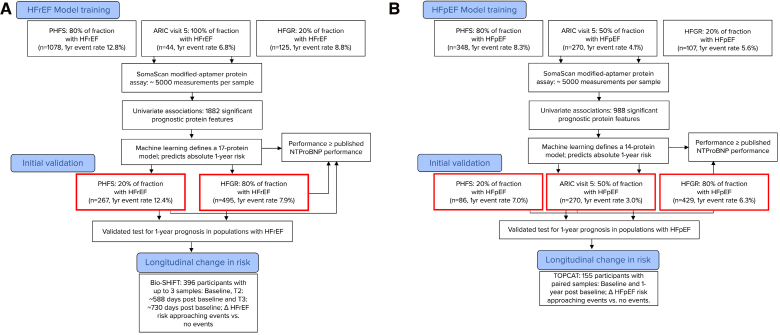
Methods: Plasma samples from individuals with HF with reduced ejection fraction (HFrEF; ejection fraction <40%; training/validation n=1247/762) and preserved ejection fraction (HFpEF; ejection fraction ≥50%; training/validation n=725/785) from 3 independent studies were run on the SomaScan Assay measuring ≈5000 proteins. Machine learning techniques resulted in unique 17- and 14-protein models for HFrEF and HFpEF that predict 1-year mortality. Discrimination was assessed via C-index and 1-year area under the curve (AUC), and survival curves were visualized. PRSs were also compared with Meta-Analysis Global Group in Chronic HF (MAGGIC) score and NT-proBNP (N-terminal pro-B-type natriuretic peptide) measurements and further assessed for sensitivity to disease progression in longitudinal samples (HFrEF: n=396; 1107 samples; HFpEF: n=175; 350 samples).
Results: In validation, the HFpEF PRS performed significantly better (P≤0.1) for mortality prediction (C-index, 0.79; AUC, 0.82) than MAGGIC (C-index, 0.71; AUC, 0.74) and NT-proBNP (PRS C-index, 0.76 and AUC, 0.81 versus NT-proBNP C-index, 0.72 and AUC, 0.76). The HFrEF PRS performed comparably to MAGGIC (PRS C-index, 0.76 and AUC, 0.83 versus MAGGIC C-index, 0.75 and AUC, 0.84) but had a significantly better C-Index (P=0.026) than NT-proBNP (PRS C-index, 0.75 and AUC, 0.78 versus NT-proBNP C-index, 0.73 and AUC, 0.77). PRS included known HF pathophysiology biomarkers (93%) and novel proteins (7%). Longitudinal assessment revealed that HFrEF and HFpEF PRSs were higher and increased more over time in individuals who experienced a fatal event during follow-up.
Conclusions: PRSs can provide valid, accurate, and dynamic prognostic estimates for patients with HF. This approach has the potential to improve longitudinal monitoring of patients and facilitate personalized care.
Keywords: cardiovascular diseases; heart failure; natriuretic peptide, brain; prognosis; proteomics.
Conflict of interest statement
SomaLogic Inc funded the costs of the proteomic assays, and Drs Chadwick, Loupey, Hinterberg, Sampson, and Ostroff and N. Kureshi are employees of the company. Dr Ganz is a member of SomaLogic’s Medical Advisory Board for which he accepts no financial remuneration of any kind. Dr Kardys received travel reimbursement from SomaLogic and Olink.
Figures


References
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79:e263–e421. doi: 10.1016/j.jacc.2021.12.012 - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Colvin MM, Drazner MH, Filippatos GS, Fonarow GC, Givertz MM, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136:e137–e161. doi: 10.1161/CIR.0000000000000509 - PubMed
-
- Canepa M, Fonseca C, Chioncel O, Laroche C, Crespo-Leiro MG, Coats AJS, Mebazaa A, Piepoli MF, Tavazzi L, Maggioni AP; ESC HF Long Term Registry Investigators. Performance of prognostic risk scores in chronic heart failure patients enrolled in the European Society of Cardiology Heart Failure Long-Term Registry. JACC Heart Fail. 2018;6:452–462. doi: 10.1016/j.jchf.2018.02.001 - PubMed
-
- Pocock SJ, Ariti CA, McMurray JJ, Maggioni A, Køber L, Squire IB, Swedberg K, Dobson J, Poppe KK, Whalley GA, et al. ; Meta-Analysis Global Group in Chronic Heart Failure. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J. 2013;34:1404–1413. doi: 10.1093/eurheartj/ehs337 - PubMed
MeSH terms
Substances
Grants and funding
- R01 HL153499/HL/NHLBI NIH HHS/United States
- R01 HL086694/HL/NHLBI NIH HHS/United States
- U01 HG004402/HG/NHGRI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- R01 HL087641/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- R01 HL155209/HL/NHLBI NIH HHS/United States
- U01 DK108809/DK/NIDDK NIH HHS/United States
- R01 AG052964/AG/NIA NIH HHS/United States
- HHSN268201700004C/HB/NHLBI NIH HHS/United States
- R01 HL059367/HL/NHLBI NIH HHS/United States
- R01 HL159081/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HB/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- R01 HL148218/HL/NHLBI NIH HHS/United States
- R01 HL129856/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
