

Small bowel obstruction secondary to strangulated obturator hernia with transected ileal segment: A case report
- PMID: 40054411
- PMCID: PMC11930148
- DOI: 10.1016/j.ijscr.2025.111098
Small bowel obstruction secondary to strangulated obturator hernia with transected ileal segment: A case report
Abstract
Introduction and importance: Obturator hernia is a rare abdominal wall hernia (<1 % incidence) that occurs through the obturator foramen, often in elderly, emaciated women. Contrast-enhanced computed tomography (CECT) of the abdomen and pelvis is the diagnostic modality of choice, with a high accuracy of 78 %-100 %.
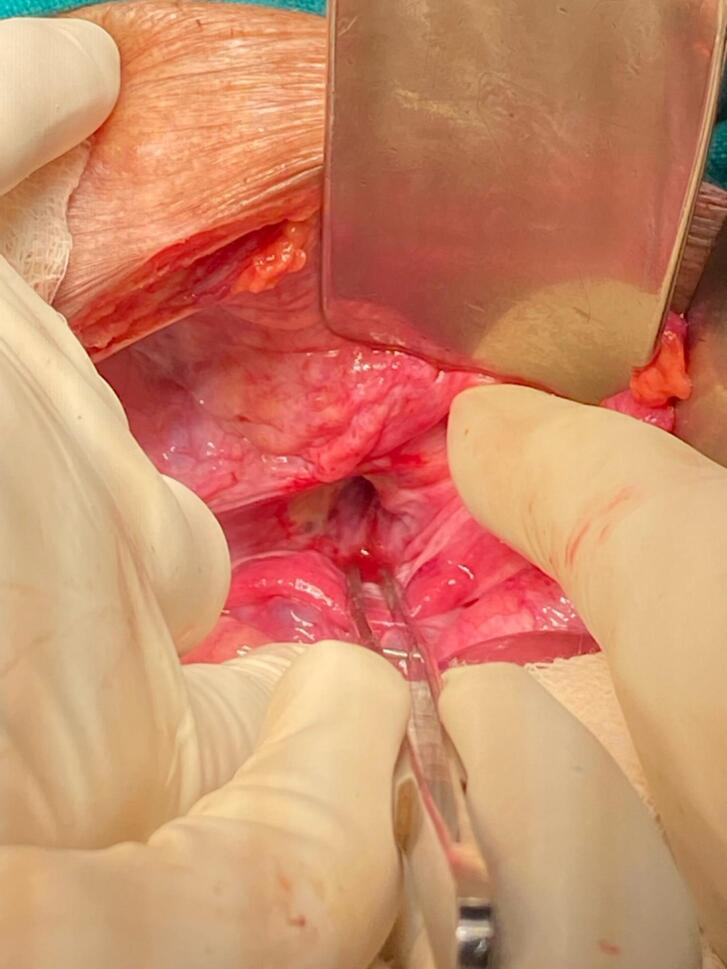
Case presentation: An 84-year-old frail woman with COPD presented with generalized abdominal pain, abdominal distention, vomiting, and right thigh pain. CECT revealed a right-sided obturator hernia causing small bowel obstruction. Emergency exploratory laparotomy revealed a right-sided strangulated obturator hernia. Postoperatively, the patient developed septic shock and multiorgan dysfunction syndrome (MODS) and succumbed to death on the 5th postoperative day.
Clinical discussion: Obturator hernia is a rare abdominal hernia with an incidence of 0.07-1 %, an often-overlooked condition, more common in elderly women (around 70-90 years) with risk factors like low BMI, multiparity, and chronic conditions such as COPD. It presents with nonspecific symptoms, including abdominal pain, distension, and vomiting, and is often difficult to diagnose. Early CECT has improved the preoperative diagnosis rate from 43 % to 90 %, thus playing a crucial role in preventing morbidity and mortality. Treatment is surgical, but the mortality rate is high due to delayed diagnosis, bowel strangulation, and underlying preexisting illness.
Conclusion: Obturator hernias are a rare but important cause of small bowel obstruction, especially in elderly, frail, malnourished women without prior abdominal surgeries. Medial thigh pain and mild abdominal distension warrant high suspicion and prompt diagnosis using CECT. Early surgical intervention is critical to prevent severe complications and reduce associated morbidity and mortality.
Keywords: Abdominal pain; Bowel obstruction; Case report; Howship-Romberg sign; Laparotomy; Obturator hernia.
Copyright © 2025 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors have no conflict of interest to declare.
Figures




References
-
- Rodríguez-Hermosa J.I., Codina-Cazador A., Maroto-Genover A., Puig-Alcántara J., Sirvent-Calvera J.M., Garsot-Savall E., et al. Obturator hernia: clinical analysis of 16 cases and algorithm for its diagnosis and treatment. Hernia. 2008 Jun;12(3):289–297. doi: 10.1007/s10029-007-0328-y. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
