

The DELIVER Technique: Deep Engagement of Guide or ChiLd-guIde Catheter for Burr DeliVEry and Rotational Atherectomy
- PMID: 40054900
- PMCID: PMC11911893
- DOI: 10.1016/j.jaccas.2024.103177
The DELIVER Technique: Deep Engagement of Guide or ChiLd-guIde Catheter for Burr DeliVEry and Rotational Atherectomy
Abstract
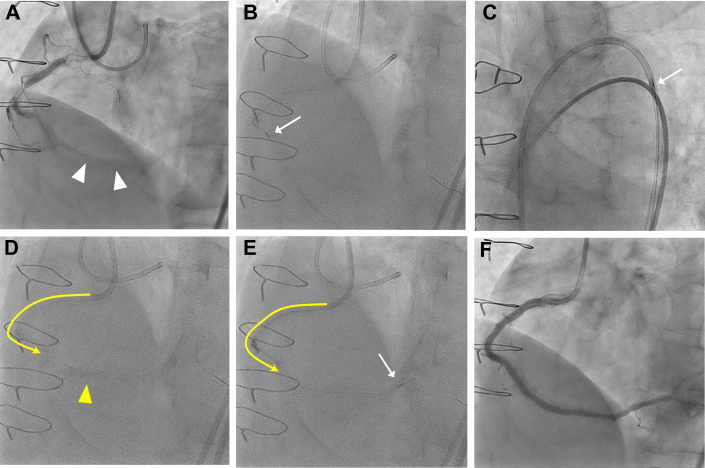
The delivery of the rotational atherectomy burr can sometimes be hindered in distal calcified lesions complicated by proximal vessel tortuosity or other obstacles. This problem may result in procedural failure or fatal complications, including coronary perforation, burr entrapment, or driveshaft fracture. To prevent these catastrophic outcomes and ensure successful burr delivery, we introduce the DELIVER (Deep Engagement of guide catheter or 5-F chiLd-guIde catheter for burr deliVEry and subsequent Rotational atherectomy) technique. This method involves deep catheter insertion beyond proximal vessel tortuosity or other obstacles, using strategies such as the distal balloon anchoring technique. Once the catheter is positioned, the rotational atherectomy burr is advanced through it to facilitate the atherectomy of the distal target lesion. This report presents 3 cases where the DELIVER technique was applied successfully to treat distal lesions. The technique enabled smooth and atraumatic burr delivery, even through tortuous arterial segments or other challenging anatomical structures.
Keywords: calcified lesion; deep engagement; distal lesion; rotational atherectomy; tortuous vessel.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Drs Kaneko, Kashima, and Kuramitsu have served as proctors for Rotablator for Boston Scientific. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures





References
-
- Shimony A., Zahger D., Straten M., et al. Incidence, risk factors, management and outcomes of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol. 2009;104:1674–1677. - PubMed
-
- Généreux P., Madhavan M.V., Mintz G.S., et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trials. J Am Coll Cardiol. 2014;63:1845–1854. - PubMed
-
- Bo Liang, Ning Gu. High-speed rotational atherectomy in coronary artery calcification: the randomized ROTAXUS and PREPARE-CALC trials. Catheter Cardiovasc Interv. 2022;100:61–71. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
