

Exploring comorbidity networks in mild traumatic brain injury subjects through graph theory: a traumatic brain injury model systems study
- PMID: 40055666
- PMCID: PMC11887189
- DOI: 10.1186/s12883-025-04102-x
Exploring comorbidity networks in mild traumatic brain injury subjects through graph theory: a traumatic brain injury model systems study
Abstract
Background: Traumatic brain injuries (TBIs) are characterized by myriad comorbidities that affect the functioning of the affected individuals. The comorbidities that TBI subjects experience span a wide range, ranging from psychiatric diseases to those that affect the various systems of the body. This is compounded by the fact that the problems that TBI subjects face could span over an extended period post-primary injury. Further, no drug exists to prevent the spread of secondary injuries after a primary impact.
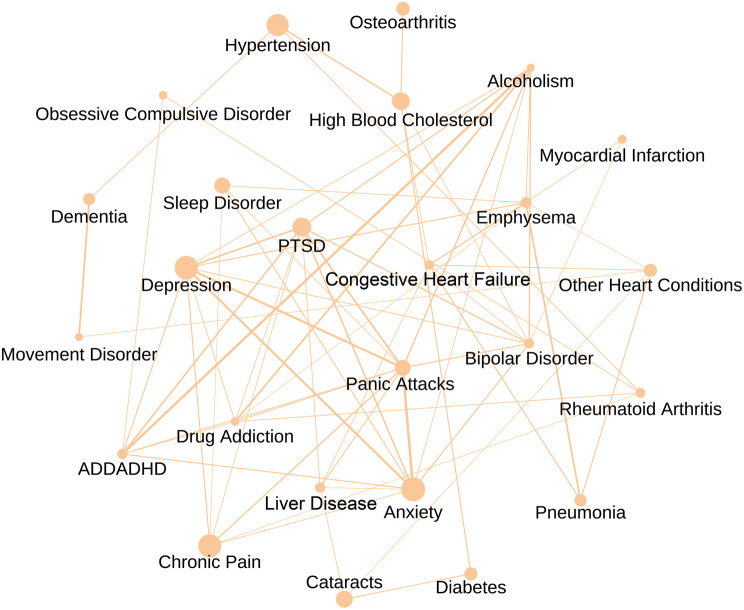
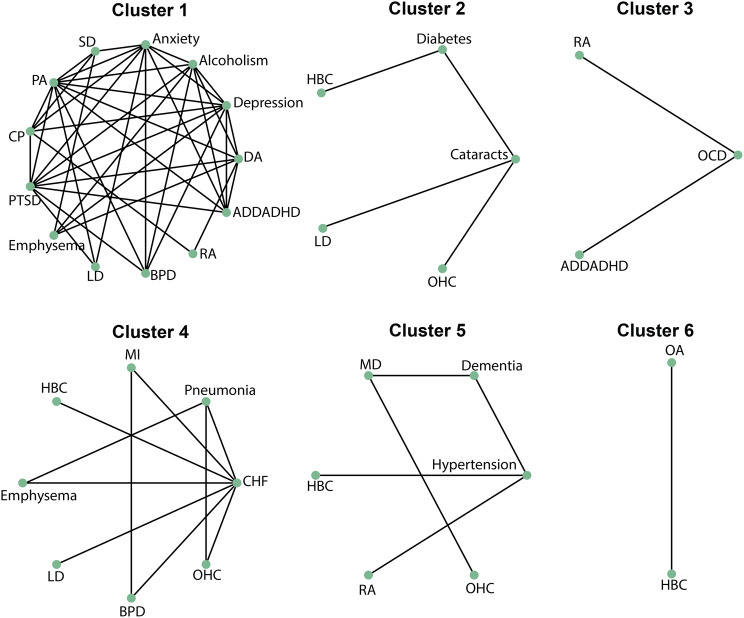
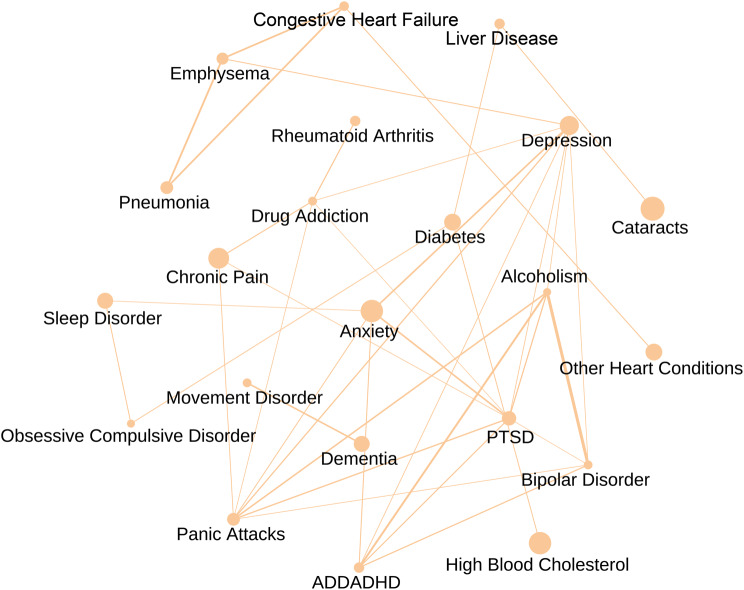
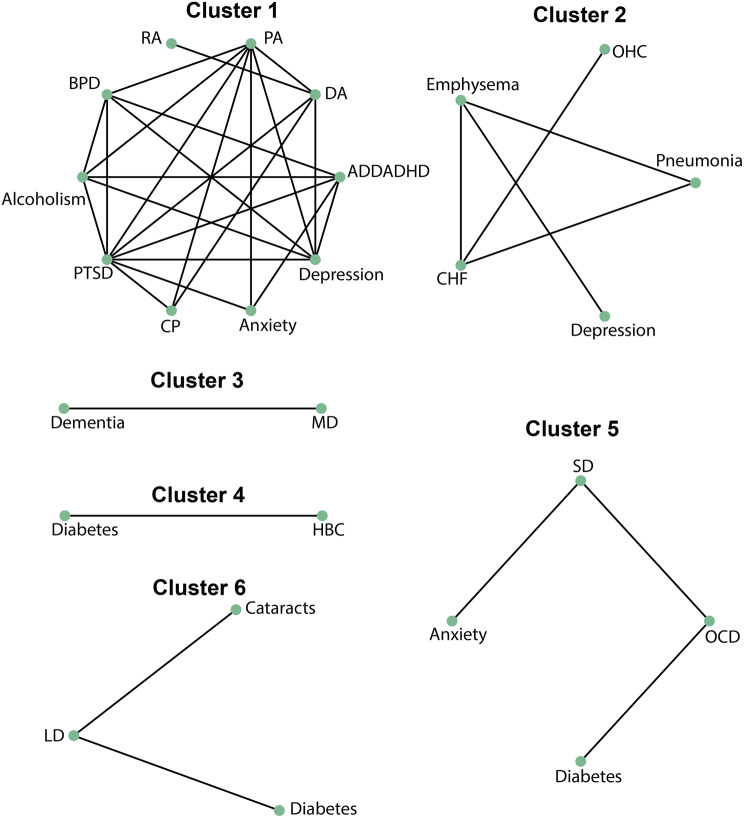
Methods: In this study, we employed graph theory to understand the patterns of comorbidities after mild TBIs. Disease comorbidity networks were constructed for old and young subjects with mild TBIs and a novel clustering algorithm was applied to understand the comorbidity patterns.
Results: Upon application of network analysis and the clustering algorithm, we discovered interesting associations between comorbidities in young and old subjects with the condition. Specifically, bipolar disorder was seen as related to cardiovascular comorbidities, a pattern that was observed only in the young subjects. Similar associations between obsessive-compulsive disorder and rheumatoid arthritis were observed in young subjects. Psychiatric comorbidities exhibited differential associations with non-psychiatric comorbidities depending on the age of the cohort.
Conclusion: The study results could have implications for effective surveillance and the management of comorbidities post mild TBIs.
Keywords: Centrality; Comorbidities; Disease comorbidity network; Graph theory; Traumatic brain injuries.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study involves secondary analysis of data of de-identified subjects and hence the need for ethics approval was waived by the institutional review board of Krea University. Informed consent is not applicable since this study involves secondary analysis of data from a database. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures




References
-
- Gururaj G. Epidemiology of traumatic brain injuries: Indian scenario. Neurol Res. 2002;24:24–8. - PubMed
-
- Maas AIR, Menon DK, Adelson PD, Andelic N, Bell MJ, Belli A, et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017;16:987–1048. - PubMed
-
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury A brief overview. J Head Trauma Rehabil. 2006;21:375–8. - PubMed
-
- Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung Y-C, Punchak M, et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. 2019;130:1080–97. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
