

Low-coverage whole genome sequencing of cell-free DNA to predict and track immunotherapy response in advanced non-small cell lung cancer
- PMID: 40055810
- PMCID: PMC11889826
- DOI: 10.1186/s13046-025-03348-0
Low-coverage whole genome sequencing of cell-free DNA to predict and track immunotherapy response in advanced non-small cell lung cancer
Abstract
Background: Outcomes under anti-PD-(L)1 therapy have been variable in advanced non-small cell lung cancer (NSCLC) without reliable predictive biomarkers so far. Targeted next-generation sequencing (NGS) of circulating tumor DNA (ctDNA) has demonstrated potential clinical utility to support clinical decisions, but requires prior tumor genetic profiling for proper interpretation, and wide adoption remains limited due to high costs.
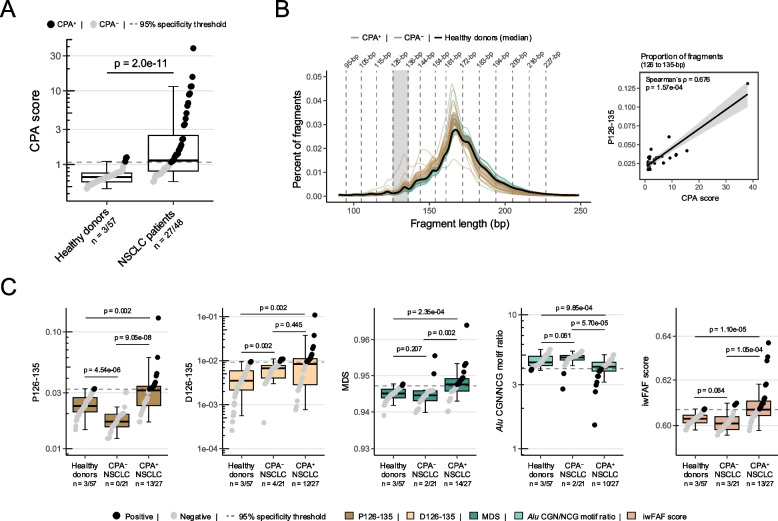
Methods: Tumor-agnostic low-coverage ctDNA whole genome sequencing (lcWGS) was used to longitudinally track genome-wide copy number variations (CNVs) and fragmentation features in advanced NSCLC patients (n = 118 samples from 49 patients) and healthy controls (n = 57). Tumor PD-L1 expression was available for comparison.
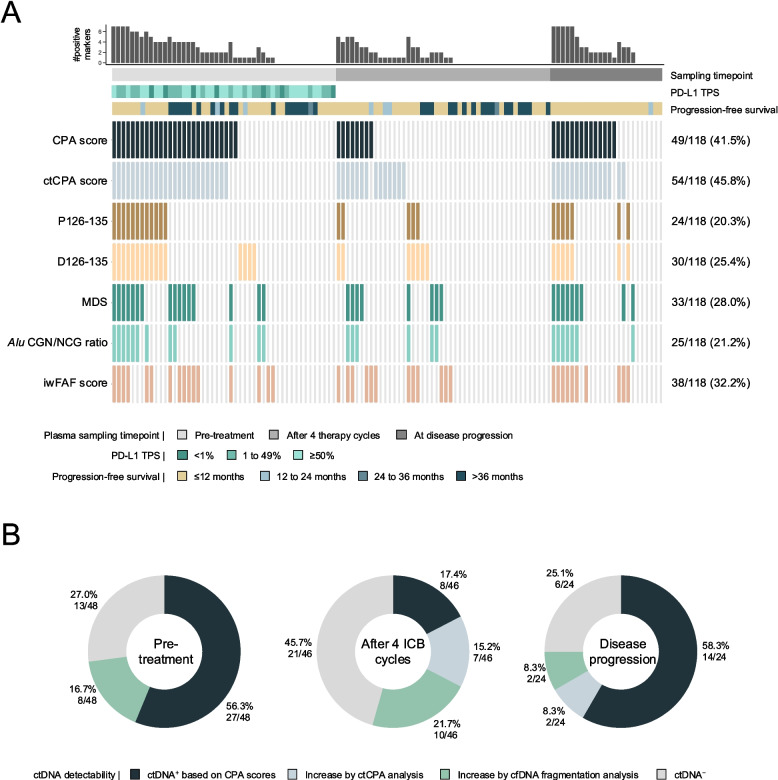
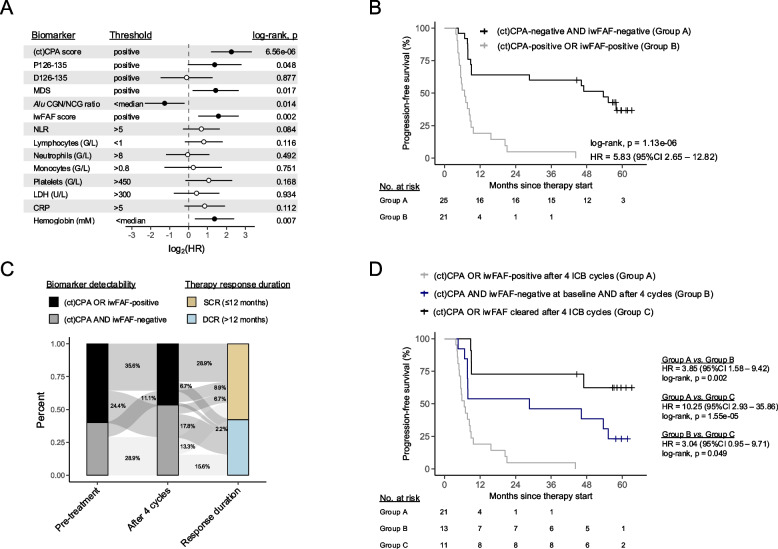
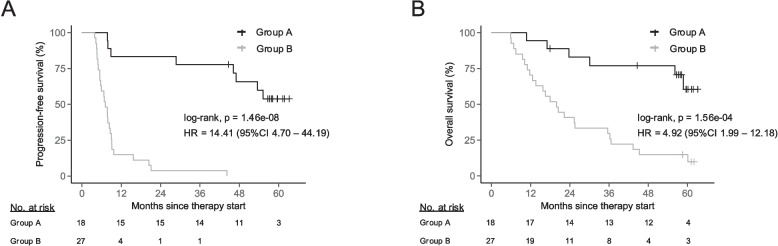
Findings: Fragmentation features and CNVs were complementary indicators, whose combination significantly increased ctDNA detection compared to single-marker assessments (+ 20.3% compared to CNV analysis alone). Baseline fragment length alterations, but not CNVs, were significantly associated with subsequent progression-free survival (PFS; hazard ratio [HR] = 4.10, p = 6.58e-05) and could improve PFS predictions based on tumor PD-L1 expression alone (HR = 2.70, p = 0.019). Residual CNVs or aberrant fragmentation of ctDNA under ongoing therapy could stratify patients according to the subsequent response duration (median 5.8 vs. 47.0 months, p = 1.13e-06). The integrative analysis of ctDNA fragment characteristics at baseline, tumor PD-L1 expression, and residual ctDNA under ongoing treatment constituted the strongest independent predictor of PFS (p = 6.25e-05) and overall survival (p = 1.3e-03) in multivariable analyses along with other clinicopathologic variables.
Interpretation: This study demonstrates the feasibility and potential clinical utility of lcWGS for the tumor-agnostic stratification and monitoring of advanced NSCLC under PD-(L)1 blockade based on CNV and fragmentomic profiling.
Keywords: CfDNA fragmentation; Copy number variations; Immunotherapy; Liquid biopsy; Low-coverage whole genome sequencing; Non-small cell lung cancer; Response prediction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the ethics committee of the Heidelberg University (S-270/2001, S-296/2016, S-145/2018) and performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to study inclusion. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016;375(19):1823–33. - PubMed
-
- Jenkins RW, Thummalapalli R, Carter J, Cañadas I, Barbie DA. Molecular and Genomic Determinants of Response to Immune Checkpoint Inhibition in Cancer. Annu Rev Med. 2018;69:333–47. - PubMed
-
- Rizvi H, Sanchez-Vega F, La K, Chatila W, Jonsson P, Halpenny D, et al. Molecular Determinants of Response to Anti-Programmed Cell Death (PD)-1 and Anti-Programmed Death-Ligand 1 (PD-L1) Blockade in Patients With Non-Small-Cell Lung Cancer Profiled With Targeted Next-Generation Sequencing. J Clin Oncol. 2018;36(7):633–41. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
