

Burr hole evacuation of chronic subdural hematoma in general versus local anesthesia: a systematic review and meta-analysis
- PMID: 40056228
- PMCID: PMC11890363
- DOI: 10.1007/s00701-025-06475-x
Burr hole evacuation of chronic subdural hematoma in general versus local anesthesia: a systematic review and meta-analysis
Abstract
Purpose: Chronic subdural hematoma (cSDH) is a highly prevalent condition that frequently requires surgical evacuation. This is typically achieved through burr hole evacuation, which can be performed under either local anesthesia (LA) or general anesthesia (GA). In the present study, we provide a systematic review and meta-analysis to study and compare the safety and efficacy of cSDH evacuation in LA and GA.
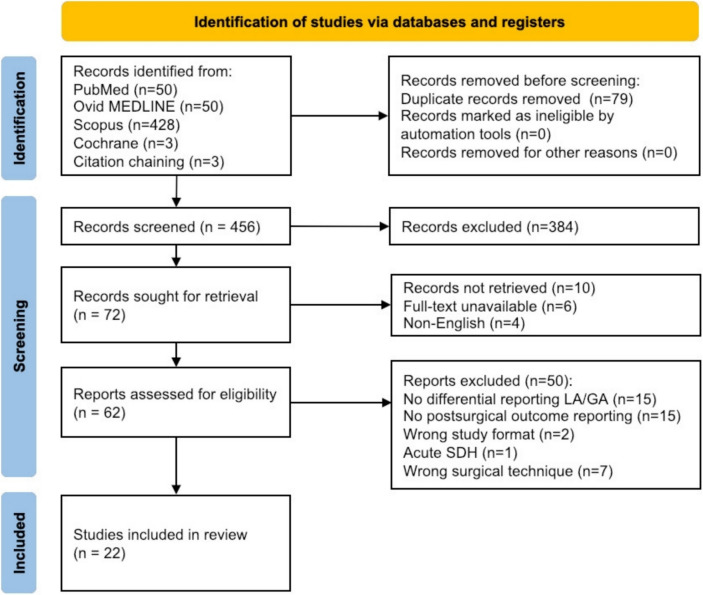
Methods: Following the PRISMA guidelines, we screened four databases for studies that compared postoperative outcomes after burr hole evacuation of cSDH in LA versus GA. Baseline characteristics and postoperative outcome data were collected, and risk ratios were calculated for each study as well as pooled across records. Random effect models were applied to continuous data points. Bias was assessed using the MINORS tool.
Results: We identified 22 eligible studies covering 3917 patients in total. LA was associated with decreased risk for complications (p < 0.001), shorter surgery duration (p < 0.001) and hospital stay (p < 0.001). There was no statistically significant association with recurrence rates, postoperative seizure or occurrence of pneumocephalus. In a subanalysis including only data from studies utilizing subdural drainage, results remained largely similar with LA proving advantageous in terms of shorter surgery duration (p < 0.001) and hospital stay (p < 0.001).
Conclusion: LA may serve as a safe alternative to GA for cSDH surgery, associated with fewer postoperative complications and providing benefits regarding shorter hospital stay and surgery duration.
Keywords: Burr hole evacuation; Chronic subdural hematoma; General anesthesia; Local anesthesia; Systematic review.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: Not applicable. Consent to participate: Not applicable. Consent to publish: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Benjamini Y, Hochberg Y (1995) Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Series B Stat Methodol 57(1):289–300
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
