

Adult Growth Hormone Deficiency, Replacement Therapy, and Outcomes in Long-Term Childhood Cancer Survivors
- PMID: 40056454
- PMCID: PMC12582300
- DOI: 10.1210/clinem/dgaf156
Adult Growth Hormone Deficiency, Replacement Therapy, and Outcomes in Long-Term Childhood Cancer Survivors
Abstract
Context: The consequences of untreated adult growth hormone deficiency (aGHD) among childhood cancer survivors are not well defined. The lack of evidence and socioeconomic factors may contribute to underutilization of growth hormone therapy (GHT) among survivors with aGHD.
Objectives: This work aimed to examine the association of GHT use with socioeconomic factors and to assess the effect of untreated aGHD in survivors using insulin-like growth factor-1 (IGF1) as a marker of GH action.
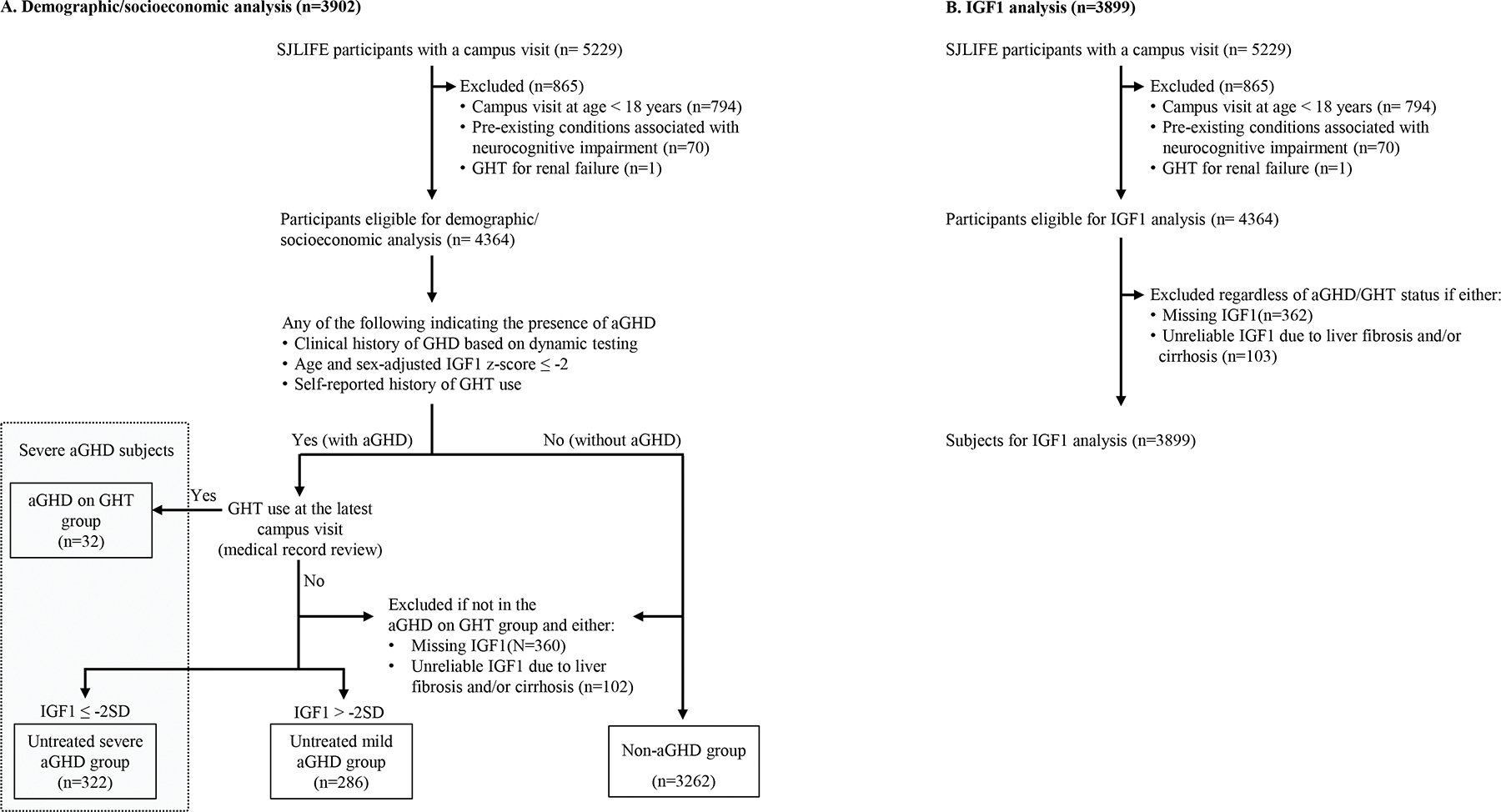
Methods: A total of 3902 five-year survivors of childhood cancer aged 18 years and older were included. The associations between GHT use and socioeconomic factors (health insurance coverage, income, area deprivation index), and associations between IGF1 levels and prevalences of adverse physical, neurocognitive, and psychosocial outcomes were assessed cross-sectionally by multivariable logistic regression adjusting for potential confounders.
Results: Among 354 survivors with severe aGHD, 9.0% were on GHT. Socioeconomic disadvantages were independently associated with less use of GHT (eg, odds ratio [OR] of GHT use 0.27; 95% CI, 0.08-0.84 for annual household income <$40 000 vs ≥$80 000). The low IGF1 group (z score ≤ -2) experienced significantly higher prevalences of various adverse outcomes compared to the normal IGF1 group (z score >0), including various neurocognitive impairment (eg, verbal reasoning [OR 2.79; 95% CI, 1.95-3.98]), diminished health-related quality of life (eg, physical functioning [1.97; 1.35-2.86]), abnormal glucose metabolism (1.82; 1.21-2.71), and abnormal fat percentage (3.16; 1.98-5.26).
Conclusion: Untreated aGHD potentially contributes to multidimensional adverse outcomes, and GHT may provide health benefits among survivors, though socioeconomic disadvantage may limit their access to GHT.
Keywords: IGF-1; childhood cancer survivors; growth hormone deficiency; health disparities; health insurance; recombinant human growth hormone.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com. See the journal About page for additional terms.
Conflict of interest statement
Disclosure Statement
The authors declare no competing interests.
Figures

References
-
- Molitch ME, Clemmons DR, Malozowski S, Merriam GR, Vance ML. Evaluation and treatment of adult growth hormone deficiency: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(6):1587–1609. - PubMed
-
- Yuen KCJ, Biller BMK, Radovick S, et al. American association of clinical endocrinologists and American college of endocrinology guidelines for management of growth hormone deficiency in adults and patients transitioning from pediatric to adult care. Endocr Pract. 2019;25(11):1191–1232. - PubMed
-
- Olarescu NC, Gunawardane K, Hansen TK, et al. Normal physiology of growth hormone in adults. In: Feingold KR, Anawalt B, Boyce A, eds. Endotext. MDText.com, Inc.; 2000–2022. 2015.
-
- Feldt-Rasmussen U, Klose M. Adult growth hormone deficiency- clinical management. In: Feingold KR, Anawalt B, Blackman MR, eds. Endotext. MDText.com, Inc.; 2000-. 2017. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
