

First trimester circulating miR-208b-3p and miR-26a-1-3p are relevant to the prediction of gestational hypertension
- PMID: 40057749
- PMCID: PMC11889763
- DOI: 10.1186/s12884-025-07349-x
First trimester circulating miR-208b-3p and miR-26a-1-3p are relevant to the prediction of gestational hypertension
Abstract
Background: Gestational hypertension (GH) is linked to an increased risk of cardiometabolic diseases for both mother and child, but we lack reliable biomarkers to identify high-risk women early in pregnancy. MicroRNAs (miRNAs) are small non-coding RNA that have emerged as promising biomarkers for pregnancy complications. We thus aimed to identify first trimester circulating miRNAs associated with GH and to build a miRNA-based algorithm to predict GH incidence.
Methods: We quantified miRNAs using next-generation sequencing in plasma samples collected at first trimester of pregnancy in Gen3G (N = 413, including 28 GH cases) and 3D (N = 281, including 21 GH cases) prospective birth cohorts. MiRNAs associated with GH in Gen3G (identified using DESeq2, p-value < 0.05) and replicated in 3D were included in a stepwise logistic regression model to estimate the probability of developing GH based on the miRNAs (normalized z-score counts) and maternal characteristics that contribute most to the model.
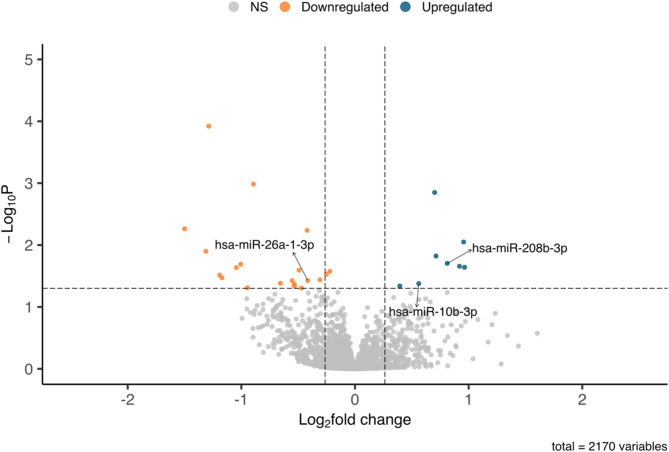
Results: We identified 28 miRNAs associated with the onset of GH later in pregnancy (p < 0.05) in the Gen3G cohort. Among these, three were replicated in the 3D cohort (similar fold change and p < 0.1) and were included in stepwise logistic regression models with GH-related risk factors. When combined with first trimester mean arterial pressure (MAP), miR-208b-3p and miR-26a-1-3p achieve an AUC of 0.803 (95%CI: 0.512-0.895) in Gen3G and 0.709 (95%CI: 0.588-0.829) in 3D. The addition of miR-208b-3p, and miR-26a-1-3p to the model significantly improves the prediction performance over that of MAP alone (p = 0.03). We then proposed low and high-risk thresholds, which could help identify women at very low risk of GH and those who could benefit from prevention monitoring throughout their pregnancy.
Conclusion: The combination of circulating miR-208b-3p and miR-26a-1-3p with first trimester MAP offers good performance as early predictors of GH. Interestingly, these miRNAs target pathways related to the cardiovascular system and could thus be relevant to the pathophysiology of GH. These miRNAs thus provide a novel avenue to identify women at risk and could lead to even more adequate obstetrical care to reduce the risk of complications associated with GH.
Keywords: Human diseases; MicroRNA (miRNA); Non-coding RNAs; Non-invasive biomarkers; Pregnancy-induced hypertension; Ribo-hormones.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study and all methods were carried out in accordance with the Declaration of Helsinki. The study and all experiments protocol were approved by the Institutional Review Board of CIUSSS de l’Estrie-CHUS (Gen3G cohort; reference number MP-31-2019-3059) and the Research ethics committee of the Sainte-Justine University Hospital Centre (3D cohort; reference number CHU-HSJ-2009-010). Written informed consent was provided by all participants involved in the study for both Gen3G and 3D prospective birth cohorts. Consent for publication: Not Applicable. Competing interests: The authors declare no competing interests.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
