

Joint assessment of abdominal obesity and non-traditional lipid parameters for primary prevention of cardiometabolic multimorbidity: insights from the China health and retirement longitudinal study 2011-2018
- PMID: 40057762
- PMCID: PMC11890515
- DOI: 10.1186/s12933-025-02667-y
Joint assessment of abdominal obesity and non-traditional lipid parameters for primary prevention of cardiometabolic multimorbidity: insights from the China health and retirement longitudinal study 2011-2018
Abstract
Background: Obesity and abnormal lipid metabolism increase the risk of various cardiometabolic diseases, including diabetes, heart disease, and stroke. However, the impact of abdominal obesity (AO) and non-traditional lipid parameters on the risk of cardiometabolic multimorbidity (CMM) remains unclear. This study aims to investigate the separate and combined effects of AO and non-traditional lipid parameters on the incidence risk of CMM.
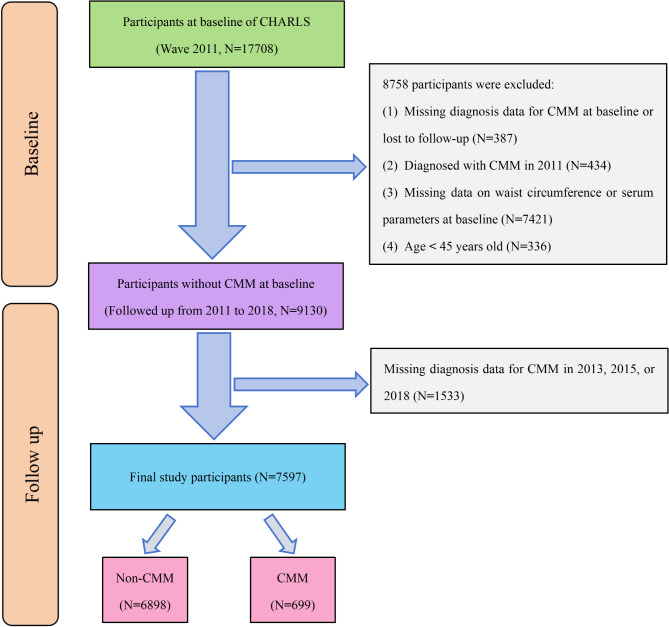
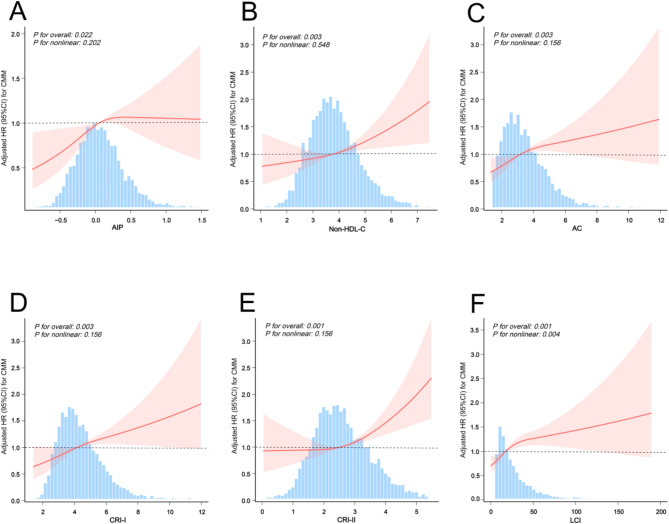
Methods: This study enrolled 7,597 eligible participants from the China health and retirement longitudinal study (CHARLS). Cox proportional hazards models were used to perform adjusted regression analyses and mediation analyses, with Kaplan-Meier analysis used for cumulative hazards. Restricted cubic splines were utilized to evaluate the nonlinear relationship between non-traditional lipid parameters and the risk of CMM among participants with AO. Subgroup analyses were conducted with stratification by age, gender, BMI, smoking status, drinking status, and hypertension to investigate interaction effects across different populations. Additionally, sensitivity analyses were further performed to evaluate the impact of various subgroups on diabetes, heart disease, and stroke.
Results: During the 7-year follow-up period, a total of 699 participants (9.20%) were newly diagnosed with CMM. Kaplan-Meier curves revealed that the subgroup with both AO and high levels of non-traditional lipid parameters had the highest cumulative hazard for developing CMM. In the fully adjusted model, Cox regression analysis revealed that participants with both high levels of non-traditional lipid parameters and AO exhibited the highest risk of developing CMM. Subgroup and sensitivity analyses further confirmed the robustness of these findings, showing consistent results across different demographic groups and under various analytical conditions. Furthermore, AO was found to significantly mediated the associations between non-traditional lipid parameters and the risk of developing CMM.
Conclusion: The separate and combined effects of AO and non-traditional lipid parameters were significantly associated with the risk of developing CMM. Notably, AO may induce CMM by partially mediating the effects of serum lipids in human metabolism. The findings highlighted the importance of joint evaluation of AO and non-traditional lipid parameters for primary prevention of CMM.
Keywords: Abdominal obesity; CHARLS; Cardiometabolic Multimorbidity; Non-traditional lipid parameters.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The CHARLS study was performed in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Peking University. All participants provided written informed consent before participating in the CHARLS study. Competing interests: The authors declare no competing interests.
Figures



References
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of Multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380:37–43. - PubMed
-
- Dove A, Marseglia A, Shang Y, Vetrano DL, Grande G, Laukka EJ, et al. Cardiometabolic Multimorbidity accelerates cognitive decline and progression to dementia in older adults. Alzheimer’s Dement. 2021;17:e050473. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
