

Altered inflammatory mucosal signatures within their spatial and cellular context during active ileal Crohn's disease
- PMID: 40059828
- PMCID: PMC11949056
- DOI: 10.1172/jci.insight.171783
Altered inflammatory mucosal signatures within their spatial and cellular context during active ileal Crohn's disease
Abstract
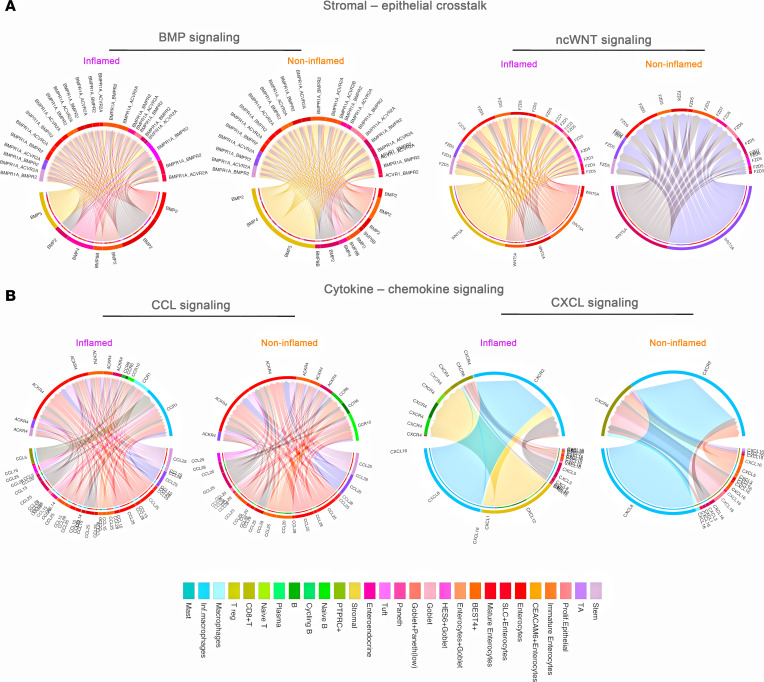
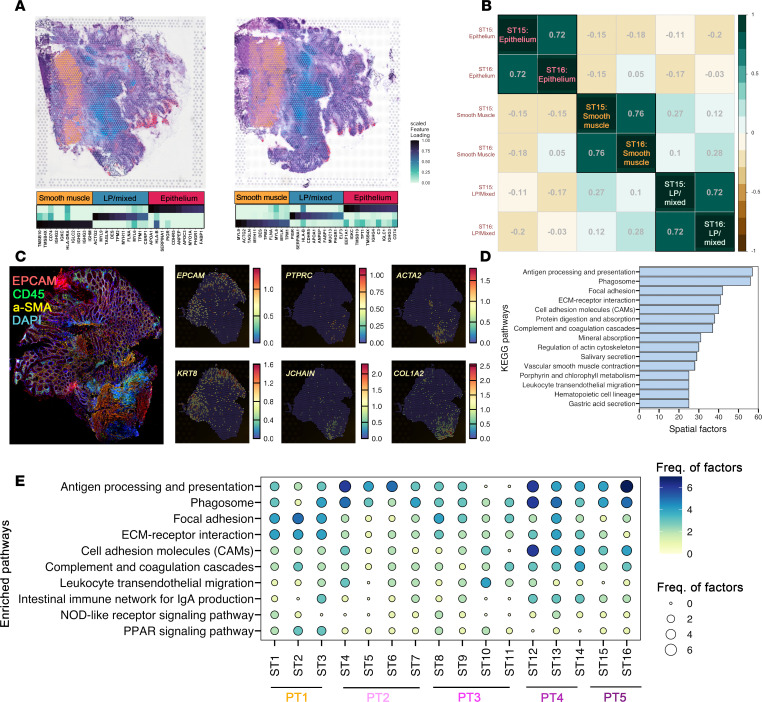
Crohn's disease (CD) involves a complex intestinal microenvironment driven by chronic inflammation. While single-cell RNA sequencing has provided valuable insights into this biology, the spatial context is lost during single-cell preparation of mucosal biopsies. To deepen our understanding of the distinct inflammatory signatures of CD and overcome the limitations of single-cell RNA sequencing, we combined spatial transcriptomics of frozen CD surgical tissue sections with single-cell transcriptomics of ileal CD mucosa. Coexpressed genes and cell-cell communication from single-cell analyses and factorized genes from spatial transcriptomics revealed overlapping pathways affected in inflamed CD, like antigen presentation, phagosome activity, cell adhesion, and extracellular matrix. Within the pathways, early epithelial cells showed evidence of significant changes in gene expression and subtype composition, while spatial mapping revealed the location of the events, particularly antigen presentation from epithelial cells in the base of the crypt. Furthermore, we identified early epithelial cells as a potential mediator of the MHC class II pathway during inflammation, which we validated by spatial transcriptomics cell subtype deconvolution. Therefore, the inflammation from CD appears to change the types of interactions detectable between epithelial cells with immune and mesenchymal cells, likely promoting the conditions for more macrophage infiltration into these inflammatory microdomains.
Keywords: Antigen; Cell migration/adhesion; Gastroenterology; Inflammation; Inflammatory bowel disease.
Figures






References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
